

sl
-
Posts
893 -
Joined
-
Last visited
-
Days Won
1
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by sl
-
-
Hi Fidelity,
I've seen patients measure their own density by cutting a square cm2 out of a piece of cardboard and applying to parts of the donor and then photographing, zooming in and counting. Ideally see some doctors as also miniaturisation, possible future loss and some specific measurements can be made, so it is more than just density readings really.
Grow your hair for a minimally week and then upload and see if it gives a clearer indication of your donor, but really in any event worth having proper consultations.
FUE scarring will depend on several factors and size and type of punches used I think would be agreed as some of the variables. Also different parts of the scalp heal differently and indeed so do patients.
I know SMP is used for linear scars, this is not my speciality so maybe others can answer about results into FUE scars and show come cases and more a question for the clinics that perform this type of work.
Body hair I never said is not a good source as such, I am just being realistic that you may need proportionally a lot more of it due to the lower hair per graft units being more prevalent.
I repeat with your loss and goals then really worth getting some personal consultations and seeing what options you have.
-
Hi amanmehra11
The graft count is correct. The hair line itself in the first few rows alone going back takes many single haired grafts and over 25 percent of the whole graft number were used and are at a higher density in order to not be to see through. Then as the transplant moves back the density is dropped as the larger hairs per grafts are deployed and the transplant is then blended into the native hair.
Depending on the loss of the patient determines how the grafts that can be placed, for more advanced loss cases then it is normal to spread the grafts more as the main concern then is coverage and we have cases whereby it is normal for 3,000 grafts to cover the frontal third of the scalp.
The further you go back then the more spreading is possible so an additional smaller amount of grafts can then go a longer way as you continue to go backwards. This is less so with hair line and smaller surgeries whereby even though you are going for an illusion, you still have to have decent graft numbers at the very front and then as said drop density as you go backwards.
Past the stage we went then you can afford to drop the density further and this is evident in post operative cases where you see the placing density diminish as it goes backwards.
As said, designs and what is wise to place really depend on the area to be treated and for cases that are more advanced then more spreading is needed, for lesser cases then one can afford to go higher density but at the cost of coverage.
So, for some 2200 grafts will do as above, on others it will go further back, so there isn't one size fits all really and several factors will need to be taken into account and some will spread further than others accordingly.
-
Hi Fidelity
Concern is that your surface area to cover is very large compared to the donor safe zone.
You are as said a NW7 and therefore could easily have 300cm2 plus area to have to work on. Your donor safe zone also is limited as the crown has dropped very deep and also the nape hair, at least from the shaved look appears to be raising up. It is certainly much lighter than the hair above it, so may be a non-harvestable area for us as a clinic. Be good as said to see grown out for a better assessment and to see how it looks.
Your safe zone from which we could take from is therefore much much smaller than the target area and as FUE takes from density we would be limited in what we could take in order not to thin out the donor too much. Clinics different on this with regard to protocol and ranging from 30 to 40 percent.
Starting density is therefore a key issue as in essence we take from this and looking at your goals it would be really wise to get your donor measured in several areas, occipital area would give the denser readings and supra auricular (above ear area) would give the less dense readings and good to measure at least 2 or 3 areas in order to get an average and not just target one area, since the FUE extractions would be spread and not concentrated.
Once you have this done then you would have some empirical data from which to see if your goals could be met.
Body hair is an extension for sure but usually the groupings are lower in terms of hairs per graft, so again many more could be needed to gain the same effect as scalp hair. If you are on a DHT blocker then it can weaken body hair, chest, leg, etc, although beard usually fairs well.
So, many things to think about and since you have specific goals then really worth having some consultations before committing to surgery and see what is possible. I have kept this brief but just an introduction to some of the things we would discuss and hopefully helpful for you.
As said you are looking at a considerable investment in terms of time and money so really worth getting it right and having some real data to go on before embarking on anything.
-
Nice write up and many good points raised.
I've known body hair on occasion also to be taken via small Strips. We haven't done it as such but have seen cases where this has been done, although in the minority and involving under arm or pubic hair, but as you say body hair is overwhelmingly harvested via FUE.
Thank you for posting, I enjoyed the read.
-
Nice write up and many good points raised.
I've known body hair on occasion also to be taken via small Strips. We haven't done it as such but have seen cases where this has been done, although in the minority and involving under arm or pubic hair, but as you say body hair is overwhelmingly harvested via FUE.
Thank you for posting, I enjoyed the read.
-
Hi Mickey85
Good questions, speaking from the patients I book personally there will be a percentage who are repair work month in month out, and that entails anything from scar work be it revisions, adding FUE or BHFUE to scars, plug removal refining hair lines etc.
I would say we see more grafting into scars than revisions per se but will speak to the other consultants also to see the percentage they book.
Scar revision per se the doctor would usually like to see the patient in the flesh as there are many variables to consider, position of the scar, laxity, fibrosis issues etc and if we feel a revision would improve the situation before opening them up again and for some FUE into scar beit scalp or beard may be the best option. Where we do revise then the doctor sutures and closes as normal.
Most patients be it virgin cases or repairs do not allow photos to be made public and the pool is smaller than virgin cases to
start with but that said I will see what I can collate in terms of revisions and scar work and will post then here.
-
Hi Stublue
Thanks for the update.
Keep washing and massaging well now and the crusts and debris will come off, twice a day is great and as you have short hair it will dry quickly.
I had occipital nerve pain for my first op ever, it does kick in a week post surgery and is more evident at night. I took iburpofen and also found massaging the donor with cold aloe vera really helped and also vitamin b to calm the nerves a bit.
Whenever guys report this to me I can tell then exactly where the pain emanates from and even that it will hurt more at night and that it will last about a week from personal experience.
The neuralgia will calm down soon for sure and as said should be fine in a week.
-
Thank you for the comments and questions.
I will see what other photos we have of the patient and information pertaining to the nature of the scar.
-
Previous surgery before in another clinic resulting in the scar as seen on the left.
Pre Surgery and placement

11 Months Post Surgery


-
Hi Hariri
Thank you for your comment.
Yes I have had a very good restoration as you say and will post mine and other cases here.
Hope everything is well with you.
-
Thank you for the comments.
For sure we have some beard cases that we can introduce to the forum.
As for the costings, I cannot be specific on individual patient cases as such but just say we have a lot of patients that come back for repeat work, I myself was a prime example of this before working for BHR I had multiple surgeries with them and as so expected that the cost depending on multiple visits and graft numbers would then decrement accordingly and not be list price, and this was my experience and very much appreciated at the time.
It is important to do this and especially so on larger cases where there is significant investment from the patient be it time, money, planning etc, and some patients have been in the chair more times than I have.
Our list prices are on our site to give a general guide but for individual surgeries over multiple visits we are happy to be more specific on any individual case.
-
Thank you for the comments.
Suturing slightly offset and slanted is fairly common nowadays and as such the doctor believes affords good closure and secures more surface area with each stitch as the doctor goes around the scar.
It keeps the closure nice and secure from experience and is done as a personal preference by the doctor although not exclusively to us.
-
Thanks for the comment and question.
For scar tissue the doctor places initially at a lower density to ensure the best chance of growth and to "break up" the scar as you say. This also primes the scar well and gives an opportunity to add again at a later stage as the vascularity improves.
Growth can be slower than into non scar tissue and I've seen cases whereby the patient gets more growth even at the 16 months stage and beyond.
This patient in particular is wearing his hair very short and traditionally the shorter the hair then the more of it needed in order to give the camouflaging effect, so could be a candidate for a second pass. Ideally we would ask for photos well past the 12 month stage and then assess from there but would expect further change from the 9 month mark.
The fact the patient does wear it shorter now shows for sure he has more confidence in doing so and is a good sign but if more is needed and asked for then we can do that also.
The only caveat on this patient is that his donor is fine and especially lower down the nape so we also need to ensure we do not make the hair in the scar too dense and also be as conservative as possible with all that we do.
-
Patient underwent several Strip surgeries prior to coming to us.
We placed 412 grafts into the scar to help camouflage it.
Patient sent 9 month update shaved to a number 1 grade.
Pre surgery

Shaved for placement


Placement

Growth at 9 months



-
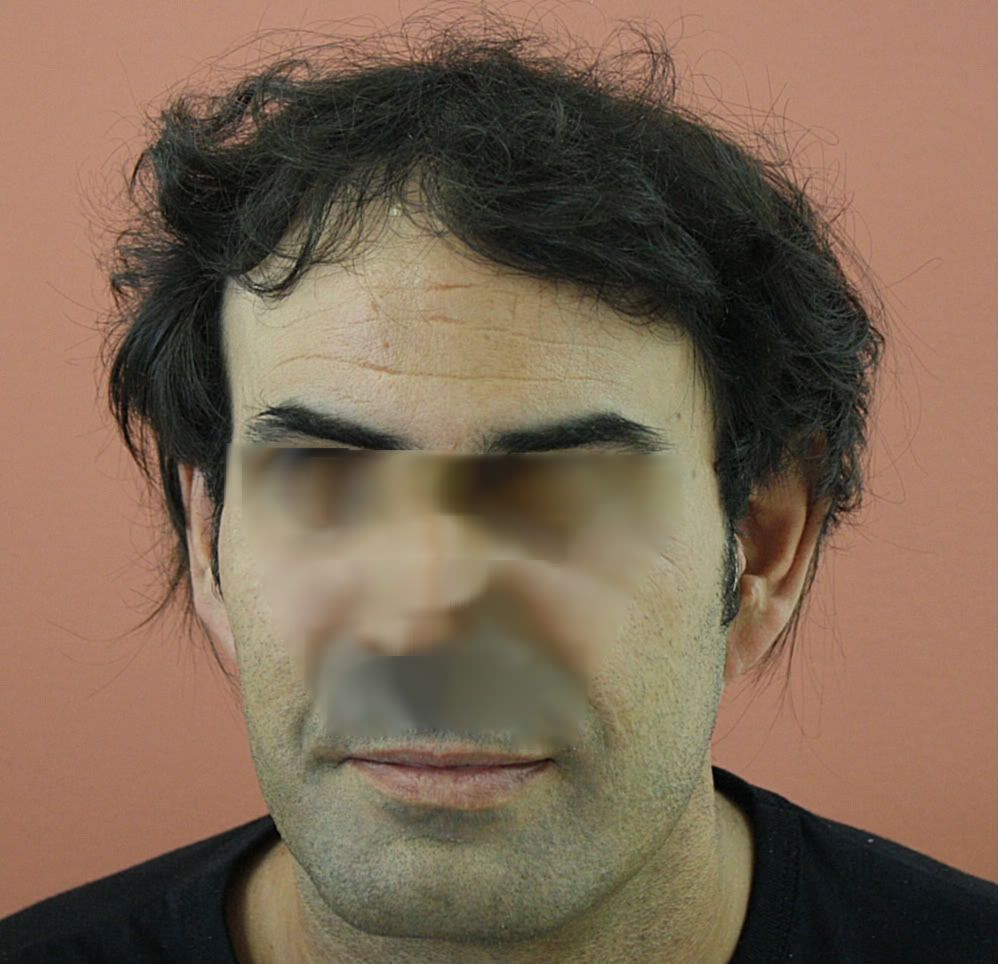
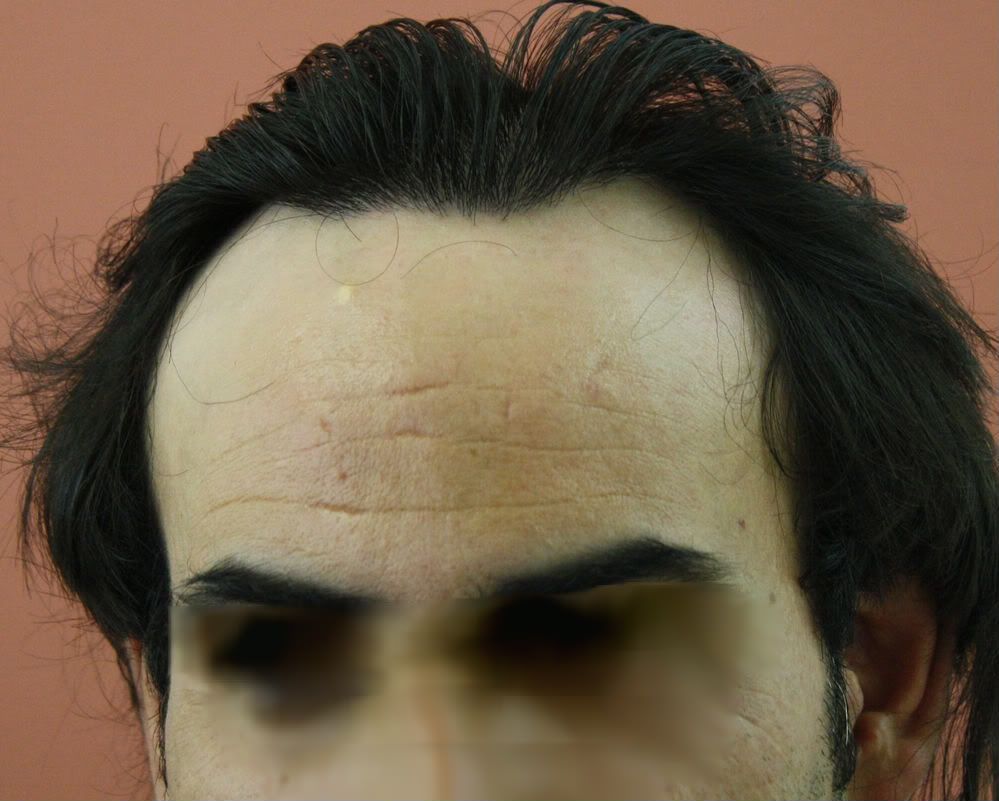
Remit for first surgery was to cover a decent area with natural looking density, designed a mature hair line that was age fitting.
First procedure goal was to achieve 4000 plus grafts with FUT.
A collage of before and after shots and then enlarged after pictures.
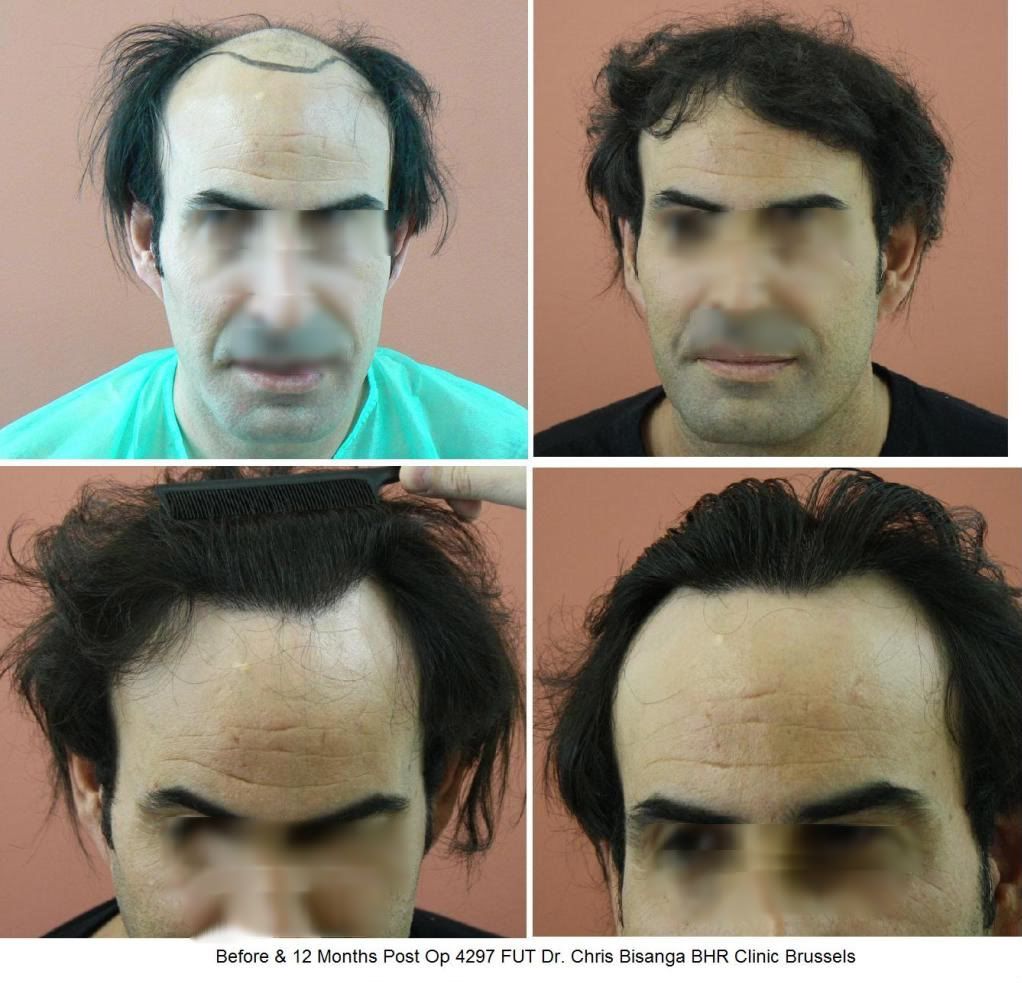




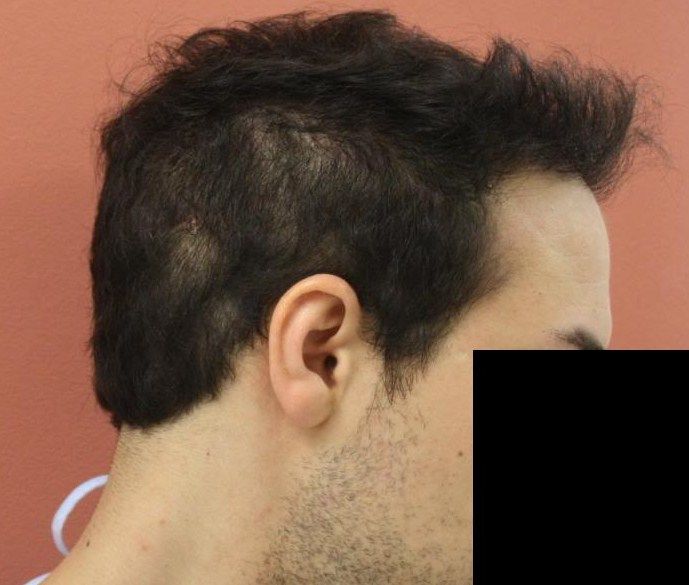
The second procedure was performed to cover the crown, with 2270 Grafts, a split between 1770 FUT and 500 FUE; the split was due to not wishing to be too aggressive with the Strip due to good healing of the first approx 4300 strip and slightly tight laxity in areas.
A small FUE allowed partial shaving and him to cover with his longer hair, also taking this option left more room for future grafts if required in the future.
Closure from first surgery.

Second Strip taken.

Crown placement


7 Months post second surgery




Final update, photos provided by patient.

A total of 15,780 hairs were placed over the two procedures,averaging to near 2.40 hairs per graft placed. A big change in appearance ensued.
-
Thank you for the comments.
For Strip I doubt we would do another one on him, this is in essence his second Strip and it healed well but we would also need to make sure he has the laxity for it also.
His donor was depleted in areas as said and I think when longer in the pre-op photos it actually looked weaker than post op.
As for the look, undoubtedly slightly longer hair helped with the illusion of coverage. There are really sweet spots whereby the hair transplant will give a better illusion at a certain length and for some cutting it short will give a different appearance as the hair is not allowed to curtain and give coverage that longer hair affords.
-
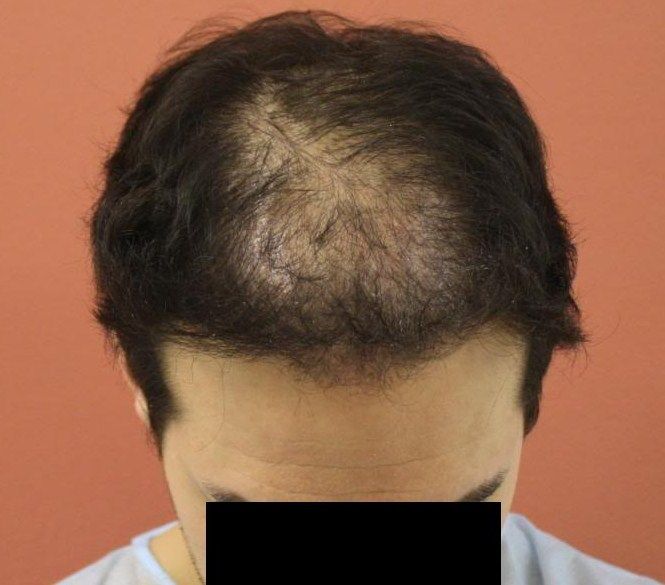
Our Patient had undergone two previously failed hair transplant procedures with other clinics. The first one he had was to rebuild his hair line using FUT and the second was to refine the hair line and then increase the coverage behind the hair line using 4000 FUE.
The second procedure caused a great reduction in the density of his donor area and poor yield in the recipient area.
We used 2716 grafts, a combination of 2056 FUT 660 FUE to refine the hair line and then improve his hair coverage in the central area. The combination was used to minimise any further changes in the donor area as the previous FUE had already over harvested and reduced the density to below average.
PRE OPERATION AND GRAFT PLACEMENT


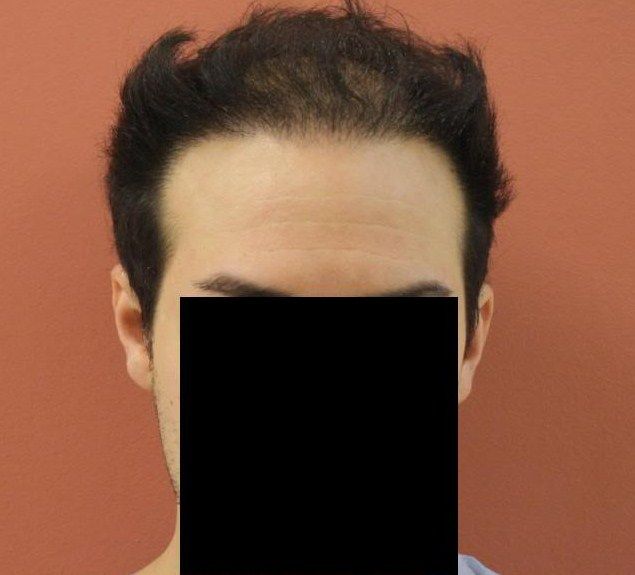

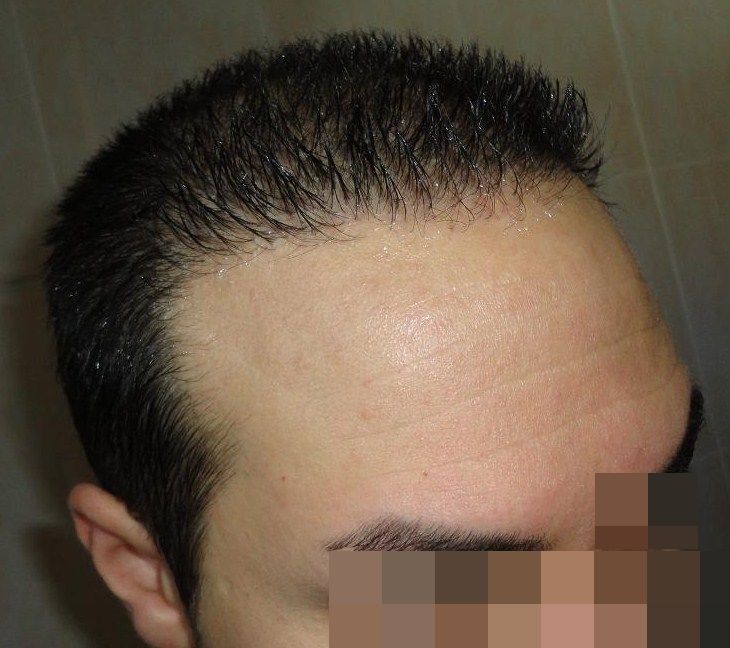
7 MONTHS POST OP AND COMPARISON



9 MONTHS POST OP


10 months update




-
Age: 32
Meds: Propecia
PRE SURGERY




DESIGN

PLACEMENT

STRIP CLOSURE

POST SURGERY 10 Months





-
Age:30
Medication : Finasteride
70 FU per cm2 average density in the donor.
Graft breakdown:-
1 hair: 608
2 hair: 990
3 hair: 585
4 hair: 17
Total: 2200
Before surgery



Placement



Update at 3 months



7 months progess

-
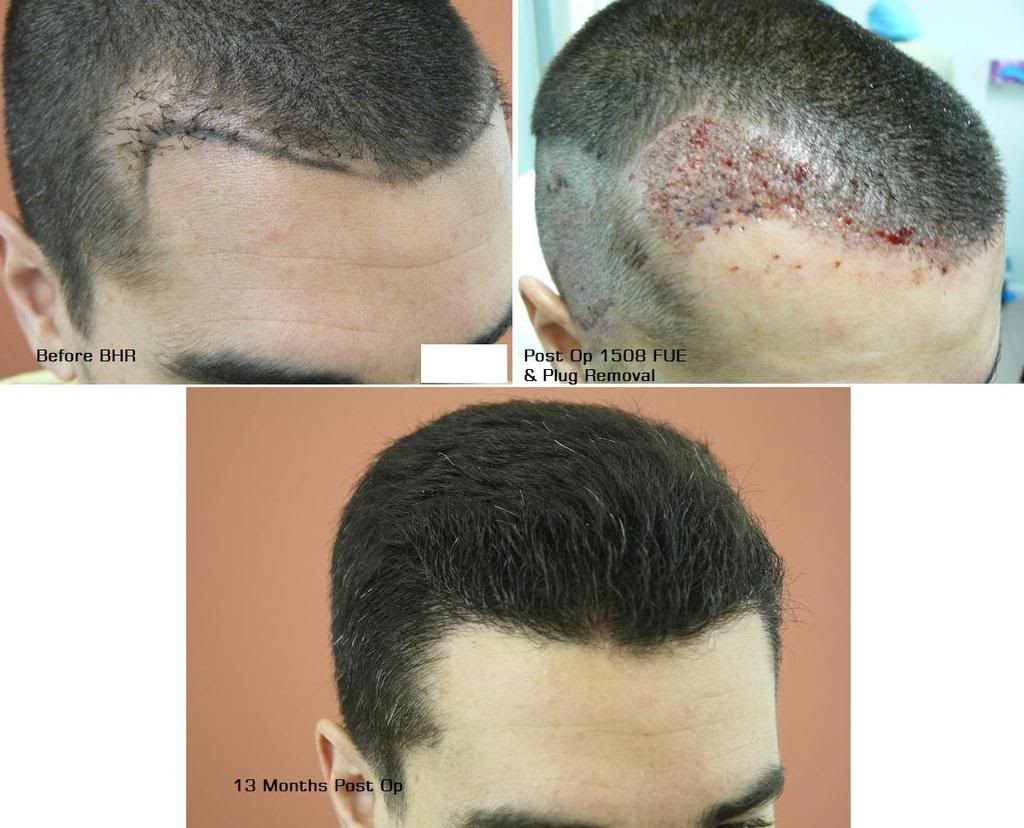
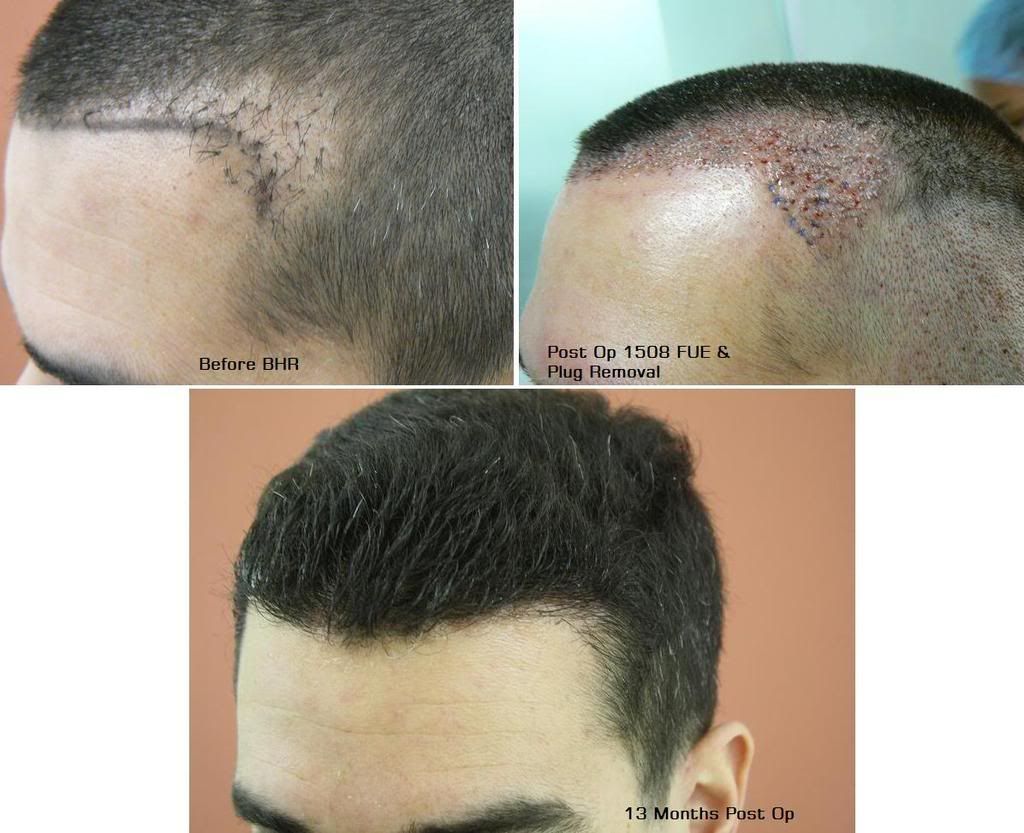
Technique FUE & Plug Removal via FUE
Graft Numbers: 1508 FUE & 95 Plug Redistribution via FUE
Time Line: 0-13 Months Post Op
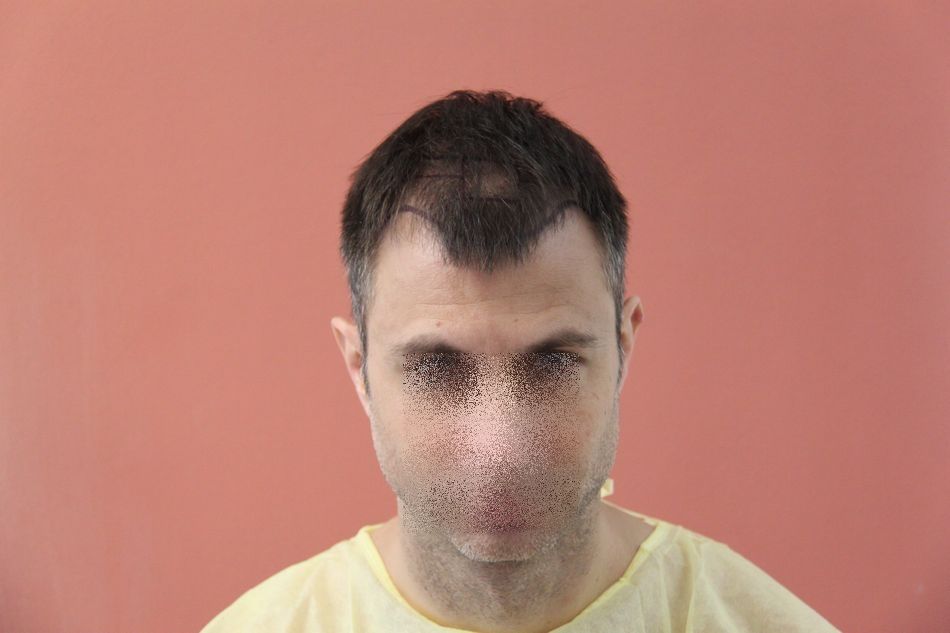
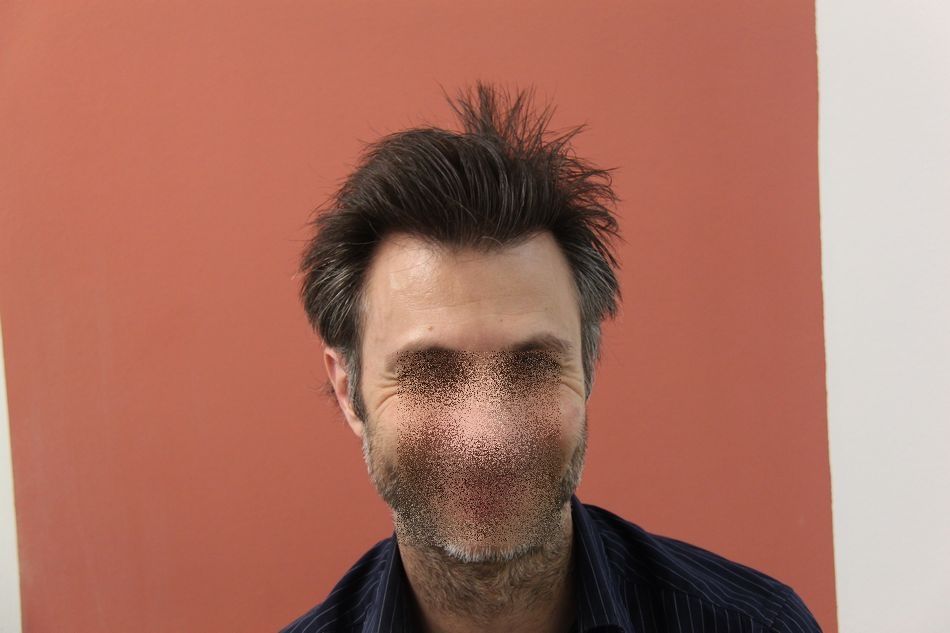
The goal was simply to repair the previous poor HT, remove or camouflage the old graft placement, slightly rebuild the very frontal line and the temples.
Pictures are Pre-op, Placement & 13 Months Post-operational




-
 1
1
-
-
Hi Stublue
Many thanks for posting, look forward to the updates and available when needed. Will keep in touch.
-
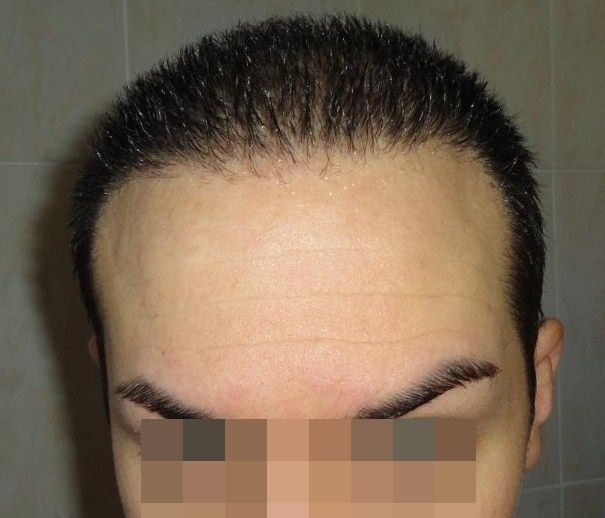
Patient Age: 38 years
Previous surgery: None
Medications: Minoxidil 5%
Density donor site: 60/65/70 FU per cm2
Hair Type: Fine
Technique: FUE
Graft Numbers: 2294
Number of hairs per graft: - 1 hair: 604 - 2 hair: 1161 - 3 hairs: 508 4 hair: 21
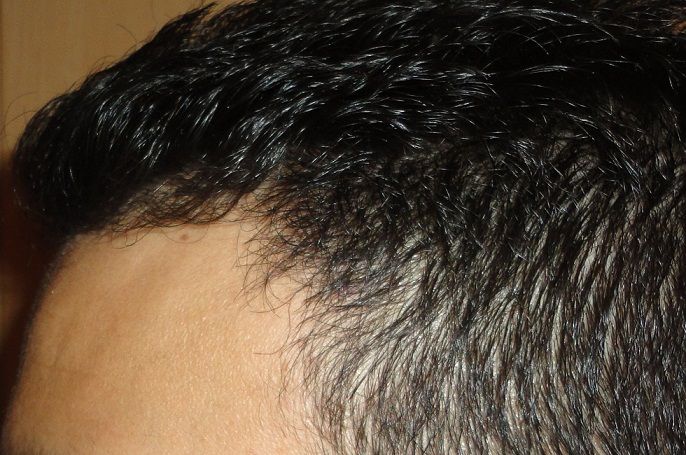
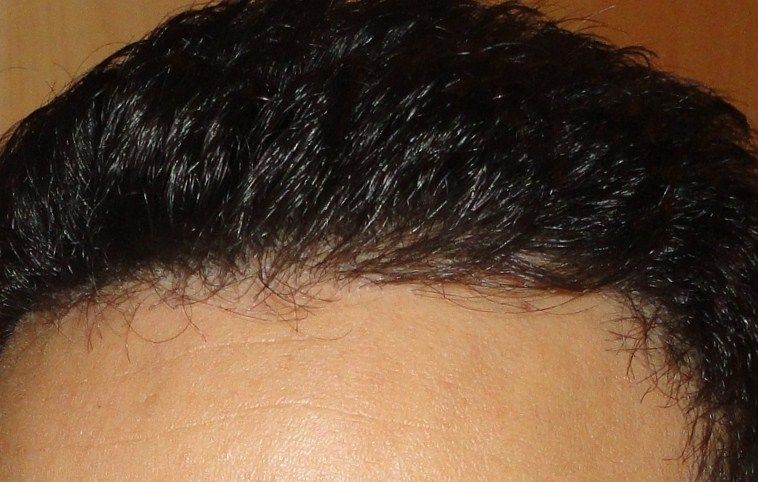
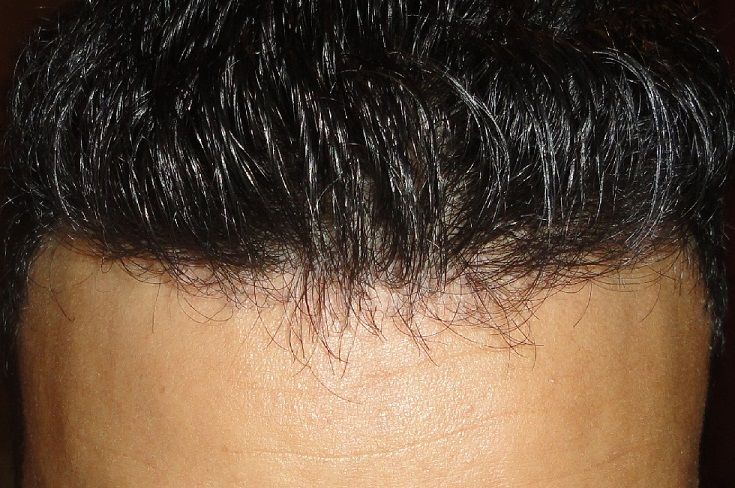
The main objective here was to re-design the hair line and blend back into the frontal third looking to improve the framing of the face and give appearance of density coverage and just behind it.
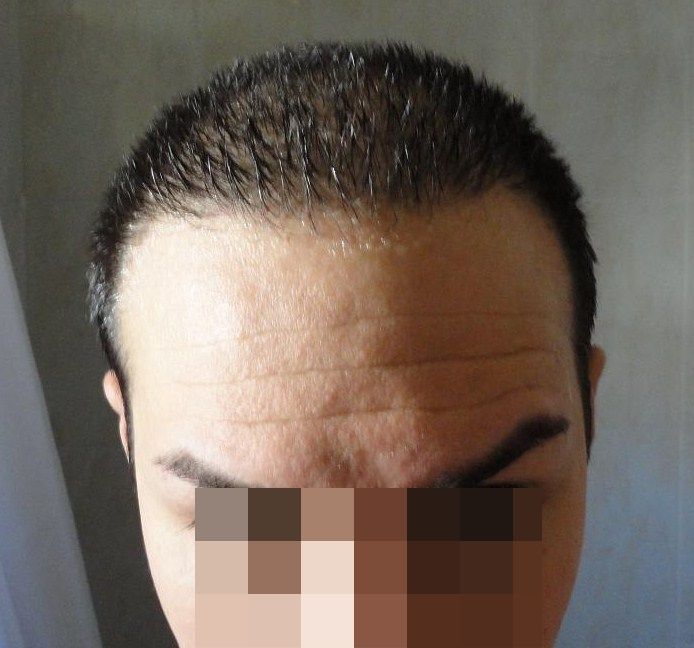
The images were taken at different angles, both wet or dry hair to document it in different conditions.
Before & Post operative 10 months.
Pre-operation.








Placement



Post op 10 Months







Dr.Bisanga, BHR Clinic, 2716 Graft Hybrid, 2056 FUT 660 FUE 0 - 10 Months
in Results Posted by Leading Hair Restoration Clinics
Posted
Thank you for the comments.
FUE takes from density so it really is a technique that needs to be spread and especially so for larger numbers, it is important to use as much surface area as possible in order to minimise the change in density and to allow a good extraction pattern so as to not choke out any particular area.
There needs to be thought in the harvesting pattern and with regards to the type of grafts needed for certain areas.
When it comes to repair work like this then it is a different ball game to some degree and the doctor needs to cherry pick and also harvest the better areas to bring lesser contrast between the over and non harvested areas. This patients donor in fact looks better post the repair surgery with more taken and also the way in which he wears his hair I think helps to bring off the change in the donor thinning.