

sl
-
Posts
893 -
Joined
-
Last visited
-
Days Won
1
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by sl
-
-
Hi Mickey
Ironically this patient was deemed a Strip candidate and indeed what we first performed on him prior to the cancer issue.
When a patient has more advanced loss and asks for FUE only then the doctor invariably will ask to see them in the flesh so we can see if their goals can be met.
FUE takes from density so this is a key issue to see how much the donor can give safely. Clinics will vary in their protocols with regards to what can be taken percentage wise. Doctor Bisanga feels around 30 percent can be taken and safely over several surgeries.
So, in essence we see what is possible with FUE alone and if this will meet their goals, be it partial or full restoration. If we feel it will not be able to attain to what they are looking for then we need to be open to other options, i.e. Strip, Strip/FUE or indeed body hair also in the mix.
At times there will need to be a compromise either on technique or coverage attainable, or simply do nothing if we feel we cannot achieve with FUE the desired result.
Some will have advanced loss and be happy with partial coverage so that in itself doesn't exclude FUE as the sole technique, so the loss and goals are evaluated before a Strip is recommended.
We see an increasing number of patients are also more open to body hair. My own case I had exceptional density but still needed to tap onto my beard in order to further my coverage and cases like this one also show what can be achieved.
One thing that advanced loss guys have to be prepared for is the time, money and a number of surgeries needed to get where they want to go. It is a marathon and not a sprint as such.
-
Many thanks for the comments.
I can say this guy even though as said has really been through a lot, he is always smiling and cheerful and a really kind positive person.
It puts hair into perspective really when you face other illness and I am happy if we can improve his life even if only by a small degree.
We will see him again and he is already calling for the next op but we need to slow him down to be honest and let nature take its course and then go from there step by step and will update again when we see him.
-
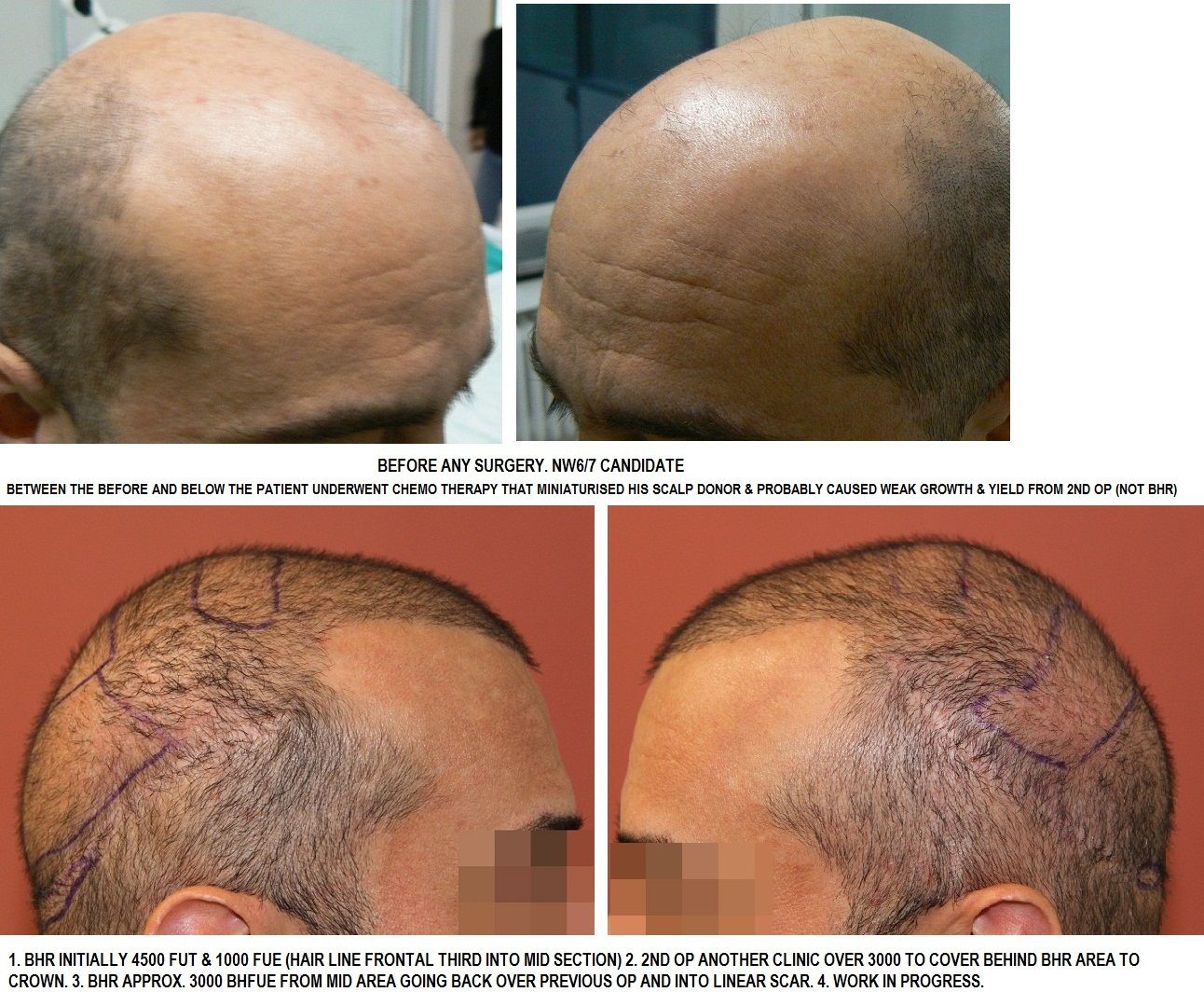
Our patient initially came to us in 2007, he was a NW6/7 candidate with average scalp donor qualities and a larger than average surface area to cover; we made an initial assessment of 2 procedures to give maximum coverage, both FUT and scalp FUE combined. The first procedure was approx. 4500 FUT and 1000 FUE; due to the surface area this covered from hair line, frontal third and slightly into the mid-section.
Unfortunately our patient was diagnosed with cancer shortly after his first procedure and had to undergo chemo therapy; this was obviously a telling time for him and he returned to us 8 months post HT op and after the therapy for an assessment.
It was assessed that the HT was growing with even coverage, although he was 8 months post op due to the chemo therapy he had growth was more like 4-5 months post op; also the donor hair was showing signs of miniaturisation so the recommendation was for he to wait at least a further year before any further surgery due to potential healing and trauma caused by the chemo reducing the yield and quality of growth.
With some understanding after beating cancer our patient wanted to have some normality in his life, although we suggested to wait he underwent a further procedure with another clinic , 3000-4000 grafts FUT, the result unfortunately was that the scalp donor miniaturised and lost density and the regrowth of the HT hair was weaker and miniaturised compared to the first procedure. This resulted in the scalp donor being depleted, the trauma caused massive miniaturisation to the extent it was in areas thinner than the recipient, the linear scar was visible as the hair would not grow over to conceal and areas of the recipient that had been treated were very thin in coverage or growth.
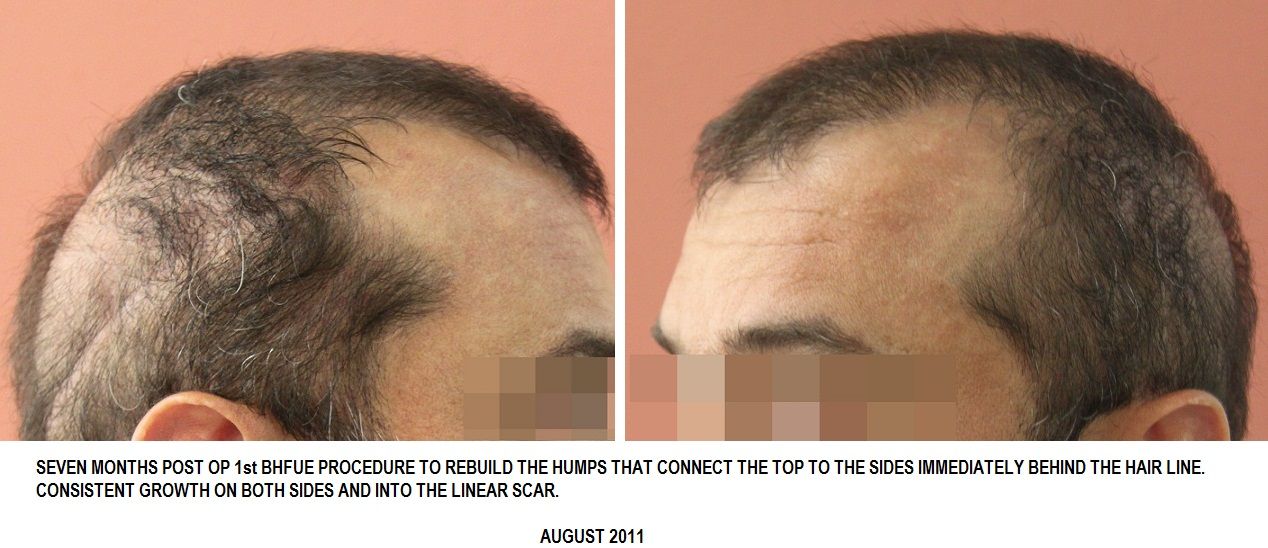
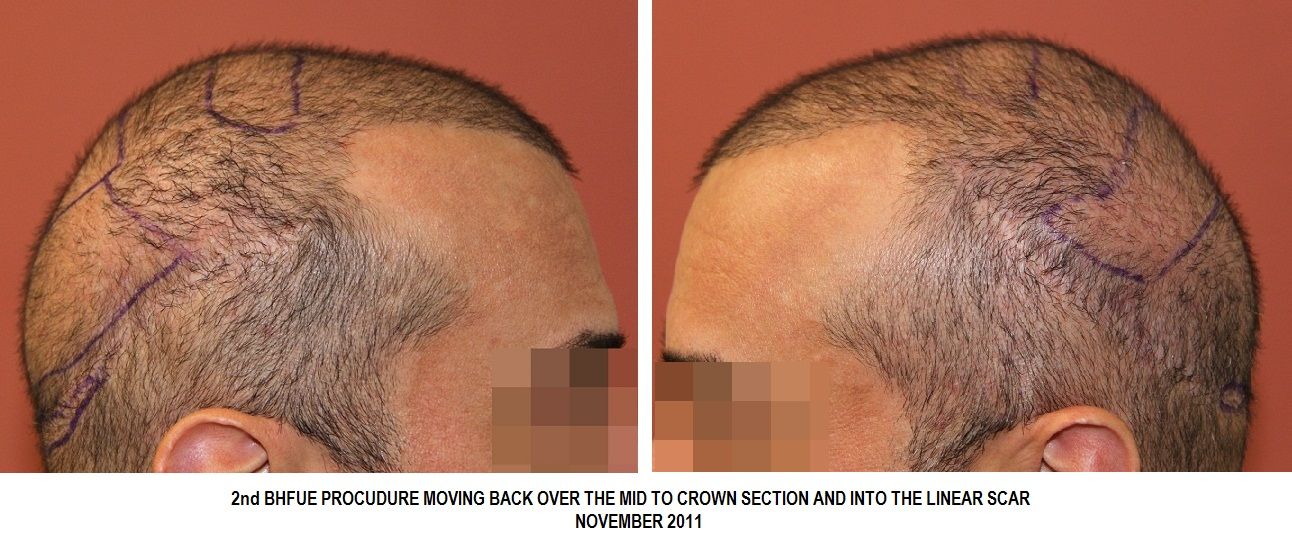
GOAL: Our patient's goal was/is to achieve maximum coverage using Body Hair, going relatively slow to ensure best yield, to start from behind the first BHR procedure and rebuild the areas that have receded and those transplanted but resulted in weak growth. The first BH procedure was in January 2011, then August and November, firstly working to rebuild the hump behind the frontal third that connects the recipient to the sides then working back further each session.
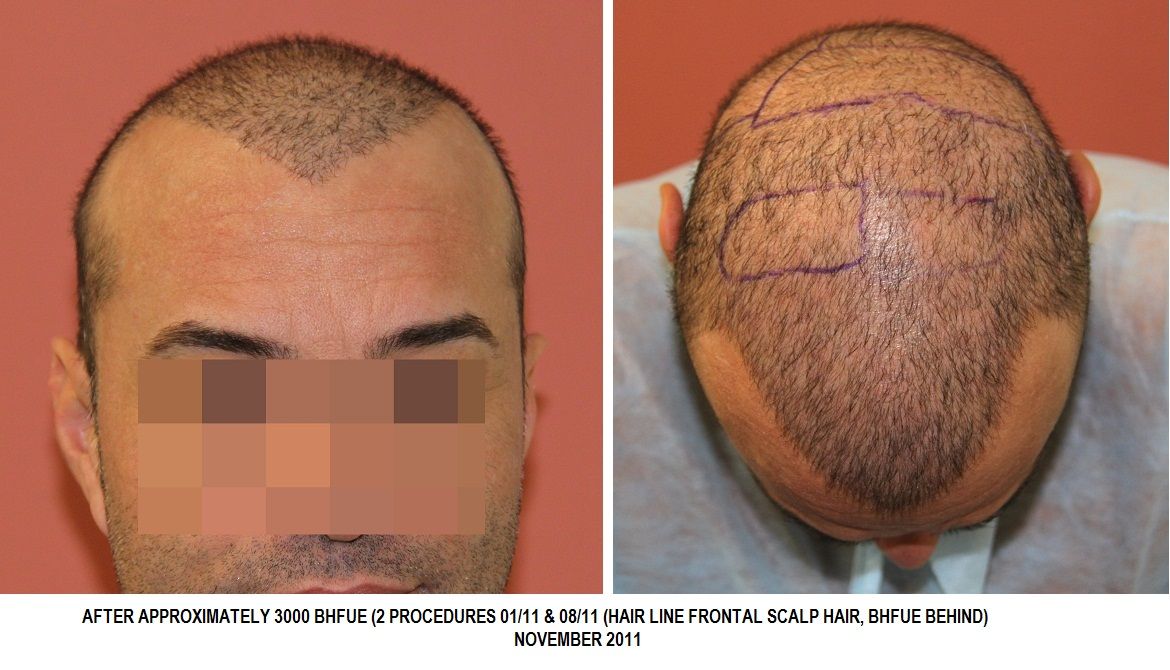
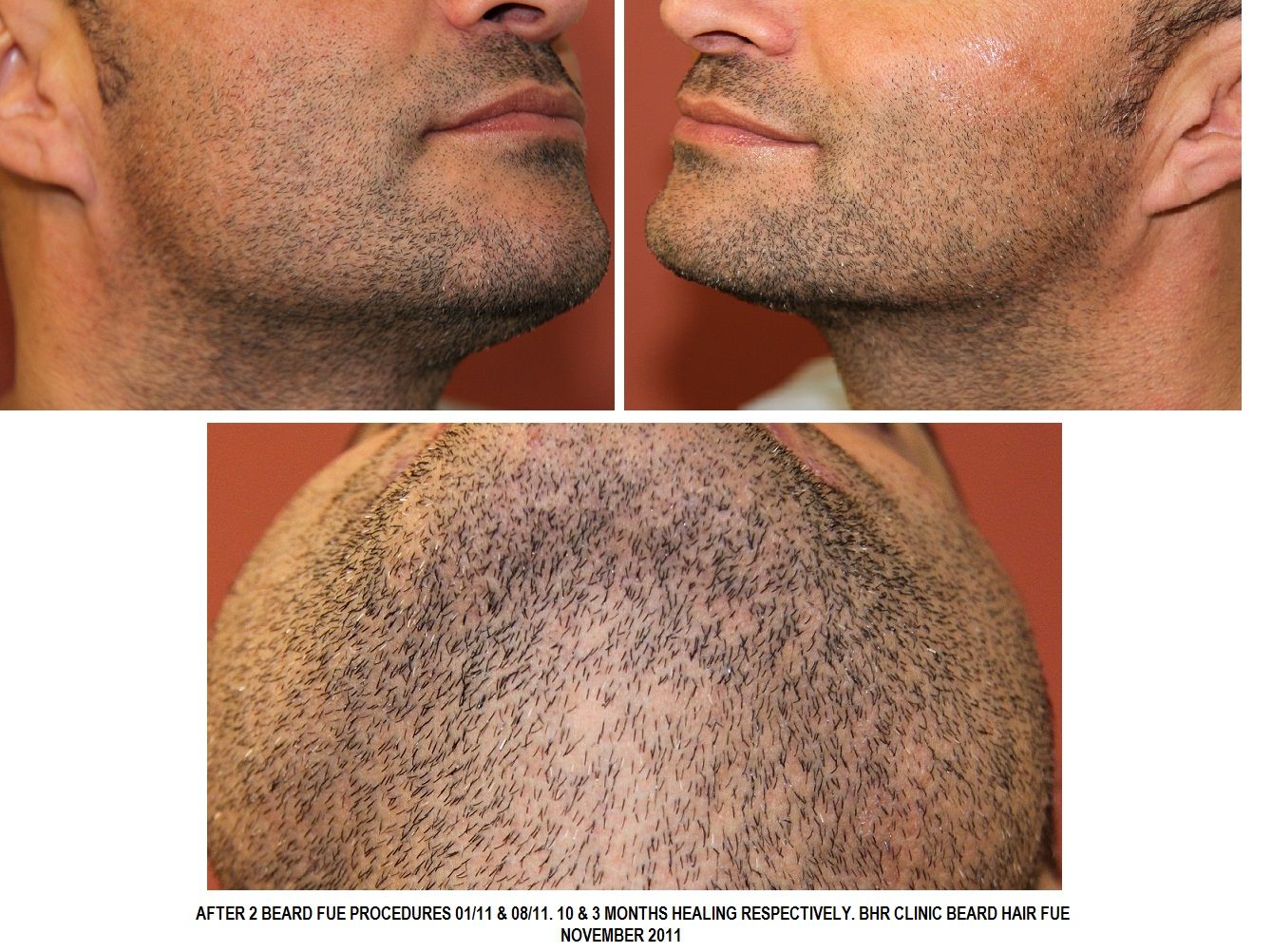
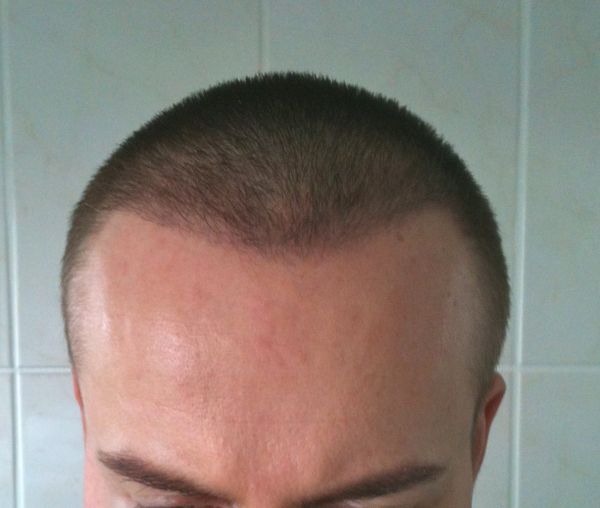
From the pictures you can see the evolution from Pre -op, to the results of Post ops and after Chemo Therapy, to Beard Hair Repair; this is on-going and we will update future ops as and when he proceeds with the goal to cover the recipient from hair line to crown, keeping the hair short so the hair blends well with his now donor area and at the same time minimise the look of the linear scar by adding hair to it.
PRE OP


APPROX. 3 YRS after 1st BHR ROCEDURE, 2.5 yrs AFTER CHEMO THERAPY & A 2nd PROCEDURE AT ANOTHER CLINIC

POST OP JANUARY 2011, START OF BHFUE REVERSAL.


UPDATE

UPDATE 2013
Patient came back for another session of body hair.
1050 grafts placed and an exact split of 50 percent of each (Chest & beard).
Chest 525, beard grafts 525
Beard healing

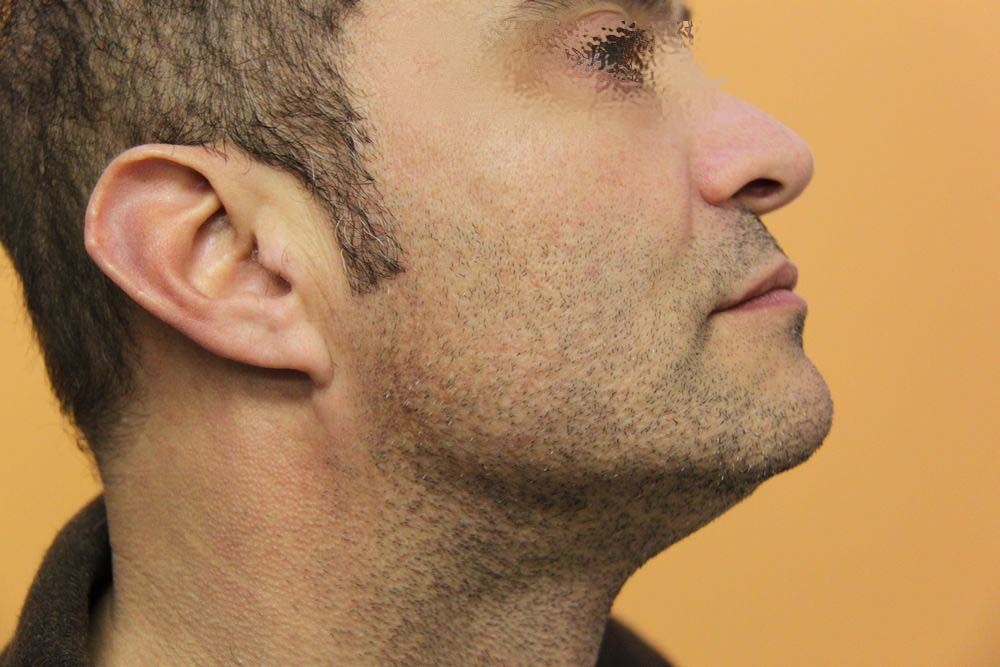


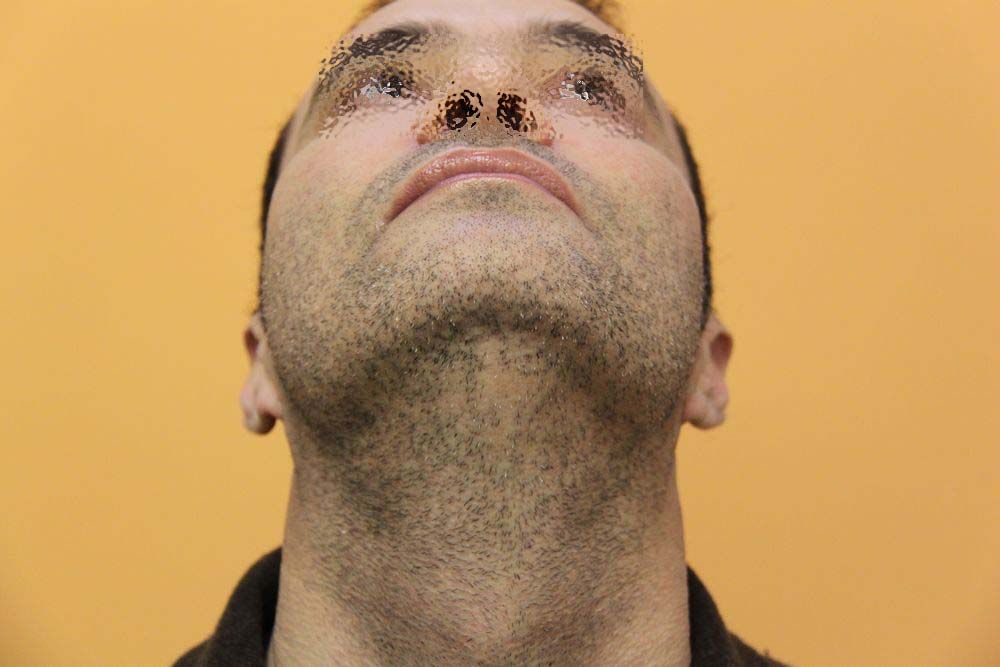
Outside photo

Indoors photos





Beard Extraction

Chest Extraction


Placement



We will update accordingly from the last session of March 2013 as and when possible.
-
Going over previously transplanted areas is not a problem as such.
If there are scarrring or pitting or ridging issues then this will need to taken into account when placing. This doesn't sound the case for you but for some who have repair work this is a possible scenario and not only the lack of density as such.
-
Nice transformation. Sure patient is over the moon.
-
I would echo looks okay at present and appears to be shock loss. Applying some minoxidil may help to speed up recovery. If you are new to it then you may wish go once a day not twice.
All the best with your healing and be patient it will take time to heal fully.
-
Likewise thanks for the photos Spex, I recall seeing it years ago.
I never personally had shockloss in any surgery but it can happen and a photo is great as it reassures patients that it can occur and that it comes back in.
-
Hi Stublu
As per phone call, some are more prone than others and this side was day 2 and you said probably had more injections there than the right side and some are more sensitive to pain on day 2 so it can then mean more injections and more risk of shock loss and therefore why on this side.
Minox once a day should help and should be on the regrowth soon and we will keep in touch but expect it to come back into life soon there and also in recipient area.
-
Leave but book a professional to remove them. Be aware than many doctors from my experience with patients have never seen anything like the length of suturing post hair transplant and some will refuse to do it through a lack of confidence and I've seen this time and again.
Poor removal will result in healing issues so it is vital to get someome who will be confident and get the clinic to also write a document as to how to remove the suture. Do your best to keep the closure clean and scab free so the doctor can see clearly what they need to do.
Cosmetic clinics per se should also be able to remove well but will do if for a price but it does beat spending two weeks in a hotel room or away from home.
-
Wise words from garageland.
I recall one patient who told me a story of waking up with his concealer all over the pillow of the girl that he had been with and then flipped it over quickly (the pillow) before leaving the house.
Must have been a real nightmare situation but he saw the funny side after but does show that the concealer can become a revealer in some circumstance.
If she likes you then she takes you as you are otherwise it could be very shallow and short lived.
Best in whatever you decide!
-
Hi Trinder
Beard grafts are usually traditionally larger than scalp, so the resulting hair is coarser and can have more curl also.
Like any transplant and even scalp hair there is a bedding in period and scalp also needs this, it can be coarser and darker than usual when transplanted and takes time to normalise, and even a few years is common as the hair goes through cycles.
The beard hair like scalp will take time to bed in and will become more refined but only to a certain degree, it is still beard hair.
I have seen hair take on the growth cycles of where placed though and have met patients whom we have transplanted scalp to eyebrows and for the first few years they are cutting the hair weekly as it grows but after a period of time notice they no longer need to cut as often as the growth phase seems to shorten and match the native hair in that region.
Likewise I have seen body hair grow long in the scalp after time as the growth phases change. It is still body hair as such though.
Beard hair for some will match very well natively and ejj and I myself are testiment to this and other posters also can confirm it has been a very compatible resource. Others may have large variations in coarseness and even colour and so it may not match as well and I know some patients with a large beard area that we have not offered surgery due to the disparity in beard to scalp and especially if the scalp hair is weak and ministurised in and around where the beard hair is needed and can be the case for scar work.
We personally ask for photos of the beard and scalp in order to make an initial assessment for compatibility and the doc may then progress to seeing the patient in the flesh and is often the case for repair work.
-
Hi Johnnydrama
I did stay on my first ones for a week but have to say it is a bit boring and especially so if you are alone. I had a lot of help from a family member so it was really much easier than patients who do come alone. Groundhog day comes to mind.
Most just want to get home to be honest.
Post operative complications are vary rare and do not really necessitate a stay for that long afterwards but I can understand those who do as I indeed did several times.
Depending on the surgery you have then it will be one or two days in the chair. Swelling is more evident by day two post op and will get worse until around day four, so best to go home before the climax of it or stay and see it out if need be and that would mean around day five for most.
For UK patients if the clinic is in Europe then the trip home is fairly easy and a few hours only and really worth just getting home in your own surroundings.
A good clinic would be in contact and easily accessible for you to air any concerns or questions while at home also.
-
Hi ejj
Seems like yesterday when we first spoke and then we saw you in the clinic for the first time.
Really happy for the improvement and especially so that new areas can be targeted and not ony "repair" areas as such and as you said to me the touching hair in these areas again is a good feeling and one that I and many can appreciate.
You have certainly been blessed with a good beard and a real "get out of jail card" and glad that some positives are coming from your whole history of surgery.
Thanks for updating and being willing to show step by step so far.
-
Hi stublue
Thanks for updating.
Work colleagues can be like that and I talk from office experience.
Normally at 4 weeks most of the transplanted hairs will have fallen and a few may not but most will and this week also therefore you will see a difference.
Minoxidil post op will help with shock loss recovery and can be applied to the donor also. I never personally had any shock loss in the donor and most don't but some do and it is usually well back by 3 months if not a bit sooner.
Liked the story, and believe me I've heard everything ranging from electric shock to blowfish poisoning and a whole host of things post op.
It is becoming more known due to the "Rooney" factor as you say and especially in the UK so can make things a bit harder for guys nowadays.
All the best for the healing.
-
The last DC consultations were January 3rd 2013 and all on my list were invited November 21 2012 as far as I can honestly see. One or two could not make due to work commitments they had and they were then promised the date for April 2013 and this is still the case and are on my list for invite as soon as we email out and this will happen in the next days.
Please do email me directly and I will check our email and see if you were invited for the last session we had there.
-
Hi recedingboy
Thank you for your comments and sorry you feel disappointed.
Dr.Bisanga does not have to see EVERY patient before surgery as such as we book patients from all continents and they do not all come to Brussels before booking surgery. There are times when he does need to see a patient in person whereby pictorial evidence is not going to address his concerns and give the empirical data needed and when we are not happy to book and take money from a patient before knowing we could meet their needs and at times this necessitates an in person meeting.
If you send me an email I would be more than happy to pull your previous emails and let you know when the doctor is next in DC. The doctor of late has not been doing regular DC consultations due to our moving clinic amongst other things and 2 to 3 times a year is maximum.
I am the English speaking rep and can promise you a timely reply and would be happy to let you know for the next DC meeting.
Of course if you have decided to go elsewhere then best wishes.
-
Thank you for the comments.
Patient's native densities were 60/70/70 FU per cm2. The lower reading being supra auricular as expected and occipital being higher.
We measure in several areas in order to get an average as the complete donor safe zone is harvested so it is good to get multiple readings and not just from one area.
We do not place hair line density higher than the lowest readings usually and so maximum would have been 60 FU per cm2 in the first few mms, possibly lower, with the single haired units and then we can afford to drop behind to 50/40 or so with larger groups deployed accordingly.
You made a good point about going into bald skin and this is often overlooked but it does make a difference.
As said it is about an illusion and not matching natural densities as such but with hair lines it is important to give a good density especially with the single units or the result can be overly see through.
Hair to skin characteristics/contrasts are also taken into account.
-
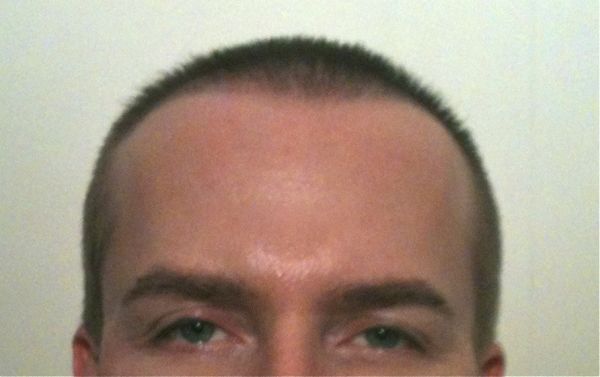
Remit was to lower hair line and give temple closure and blend back into native hair.
Age: Approx 40
Patient documented growth from inception through to one year.
Pre-surgery

Placement

At one week post op

Three Weeks


Three Months


Four Months
Six Months





Seven Months







Nine Months

Twelve Months





Full face photo

-
Those are my photos, I would recognise that shirt anywhere!
Correctly said I had all FUE and beard also placed into the crown area.
All the best dafobulous1 in whatever choice you make.
-
Hi hairtodaygonetmrw2
Good question.
We see patients who have had previous Strip surgeries and wish for more. If the scar is too high then there is a risk also that the hair there is non permanent if taken from the non save zone, and in such cases the surgeon cannot take from there even though the original scar may be there. Yours doesn't sound as if this is the case for you but the surgeon had other concerns.
The other scenario is whereby the scars are too low, this also can be in danger of being exposed if the patient were to suffer from retrograde alopecia and thus expose the scar, or, simply too low for the doctor to excise and there is a risk of stretching due to the position.
Doctors will generally try to avoid giving an additional scar but sometimes their hands are tied, or they may be able to do a partial excision if parts of the scar are in a safe area.
Without seeing photos then hard to really speak for your case other than to give some reasons as to why doctors do need to cut again and elsewhere.
-
Thanks for the update Fidelity.
You do have a very limited safe zone to take from with FUE and as said a lot to cover.
Growing the hair out a little does show more and based upon the pictorial evidence then it unless you are going to go for a lot of body hair as well then you will not get the coverage you need from scalp alone.
Creating just a hair line in itself may not look natural, you look natural now, so I would certainly think twice before doing that or anything.
-
Hi Hariri
This patients scar is very large as you say and the result of poor surgery. A revision as such was not the plan or desire of the patient as far as I am aware after asking the rep who dealt with this patient personally.
I meet many guys who have had such bad experiences and they would never dream of being opened up again due to the first experience. Simply not an option for them even if medically possible and advisable. Not all but many are like this and especially so with scars this size.
Before we revise a scar the doctor will look at the scar position, fibrosis issues, laxity, etc. If there is a good chance of stretch back then we would go for the option of FUE into it as a more secure option, or beard FUE into scar if possible.
With the width of this scar then very unlikely we would have agreed to a revision even if the patient asked for it. I can only speak for BHR clinic so I don't know the standard protocols of other clinics and if they would have offered a revision on a scar of this size as the first plan.
Many times with such poor Strip surgeries the previous doctor has also gone too deep into the tissue when taking, so there are really complications we would sooner avoid if possible.
This patient was very young and with very minimal loss and should not have had surgery in the first place, let alone a Strip, and we for sure would not have offered it where there is minimal temple loss only and young.
The result was this Scar in the donor but also very poor temple design with large plugs and several other complications I have not gone into.
If I have permission then I will also add the temple photos so show some of what I am describing. So, in short a very bad experience for the patient and he just wanted to get some "normality" back in his life.
-
In regards to the questions asked here:-
No Acell was used on this patient when he had his original Strip, it was just a very poor surgery and actually he had many complications not shown in these photos.
We will have updates form the patient to come and I will post them accordingly with the hair down.
-
Looks great Mick and I recall seeing him in the chair for the live link and enjoyed the transmission and the questions and conversation.
Great result so far and am sure he is really happy with the result at this stage which is still very early.
Dr B Farjo 4063 FUG
in Results Posted by Leading Hair Restoration Clinics
Posted
Nice hair per graft groupings and coverage. Look forward to the updates and sure it will be top drawer.