
.jpg.c593e947820640da4e1074729478c430.jpg)
H & W Doug
 Elite Coalition Physician
Elite Coalition Physician
-
Posts
431 -
Joined
-
Last visited
-
Days Won
1
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by H & W Doug
-
-
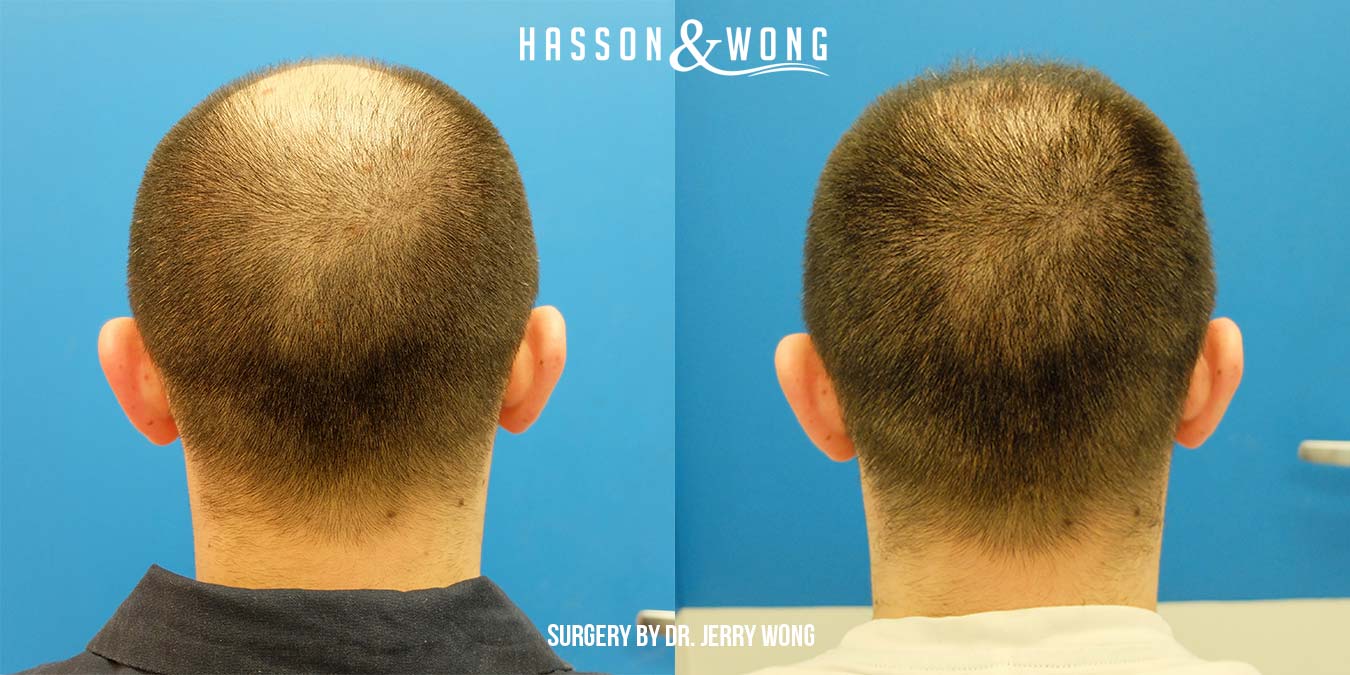
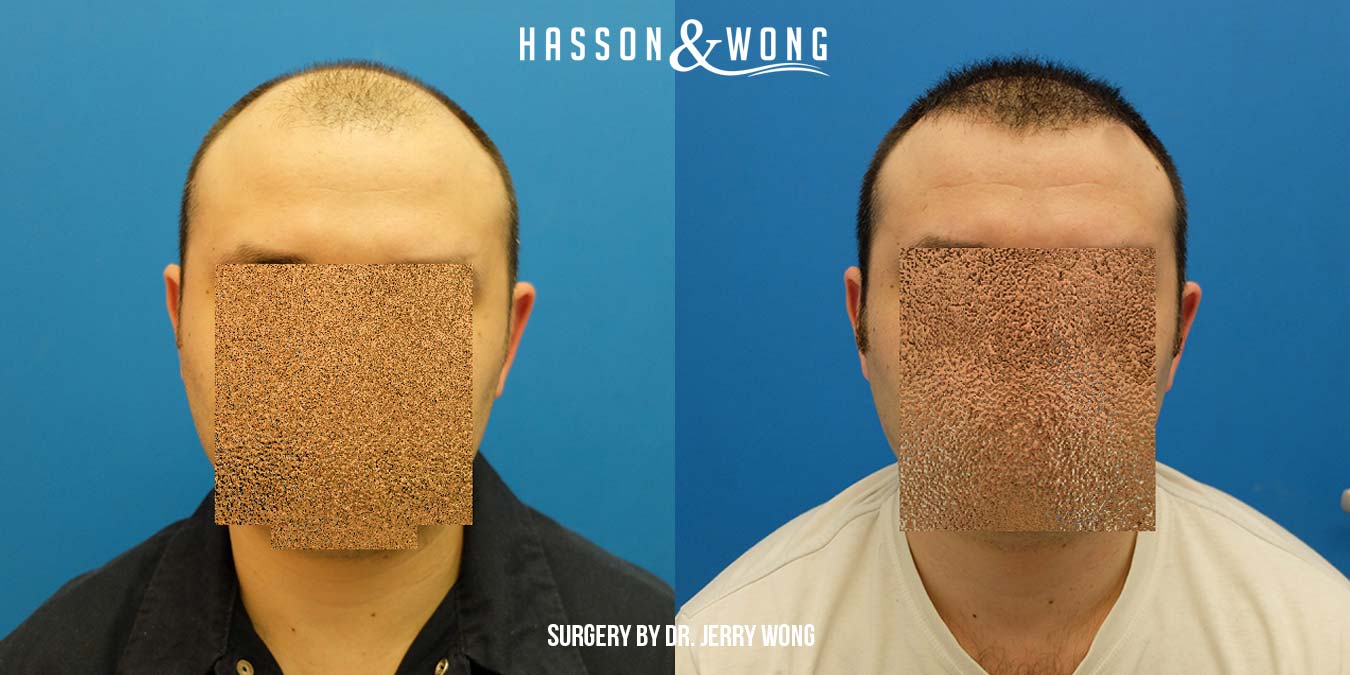
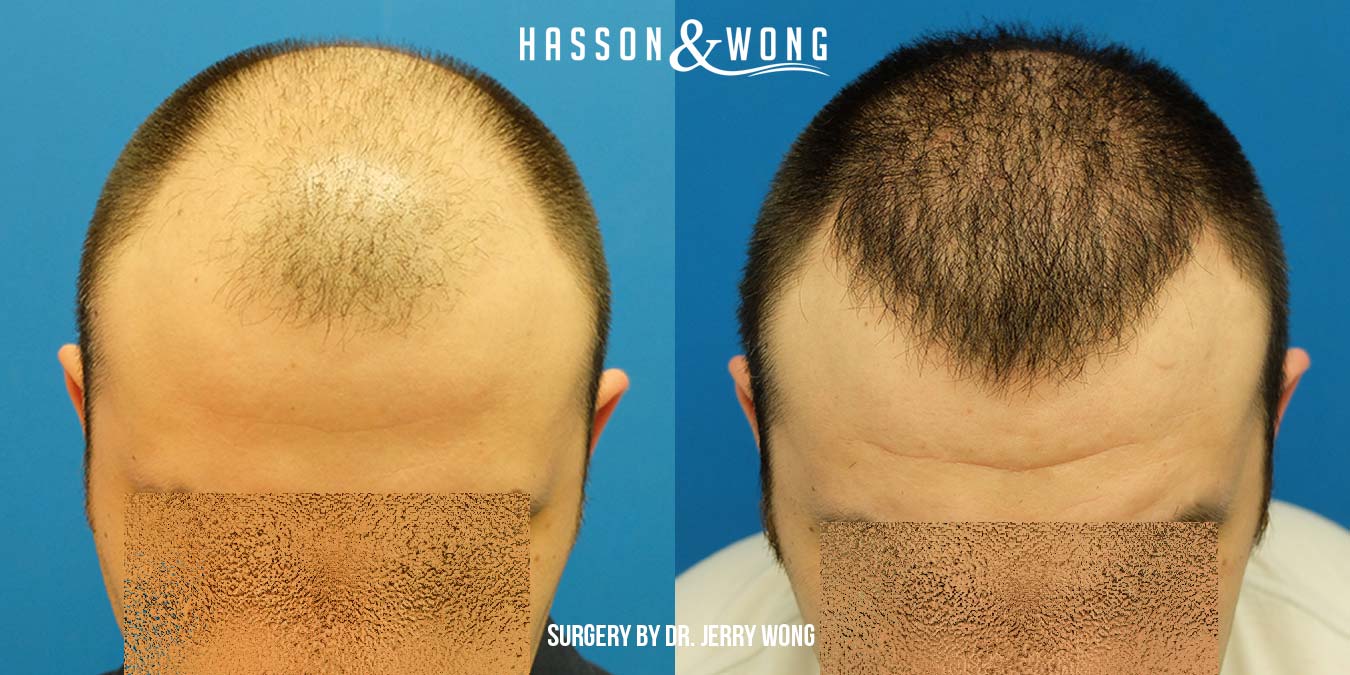
Vancouver area patient in his 60’s with fine to medium texture hair. Dr. Wong and team transplanted 4138 grafts in one session comprised of 917 single hair grafts, 2865 doubles and 356 Multiples. These photos were taken at the clinic 1 year post-op.








-
TP,
The transection rate in this case looks to be about 3%.Each doctor has a different team. Not too often but in some cases one or two members of one team will assist in a surgery for the other team depending on a few factors. I hope to have an update on this patient at some point. Dr. Wong estimates the average patient’s donor bank for FUE to be 5,000 to 7,000.
Harebrained,
In this case the patient was very certain he did not want to undergo an FUT procedure which I believe to be based in large part to not wanting a linear scar
-
Thanks trashpanda!
I think FUE first and FUT later makes sense in some cases especially if it is a relatively small amount of grafts in the first procedure most likely confined to the hairline or frontal zone. If there is a future need for a large number of grafts, FUT can be utilized later. You could make the case this line of thinking may suit a younger guy. If the doctor expected a future FUT would be a distinct possibility, in planning for this he could chose to leave the area of the potential future donor strip a little less harvested to increase the strip yield.
-
Shampoo!
I hope you are doing well.
James will be seeing patients at:
NYLO Dallas South Side
1325 S Lamar St
Dallas, TX
75215
He said he would try and meet up with you guys. I'll try and get a hold of you tomorrow, is the info from your chart current? You can also email me at doug@hassonandwong.com.
Is one of the alums the great KK of real estate fame? Tell him hi for me!
-
Well said densedream.
I have often delivered a similar message to patients over the years who were concerned about the scar.
-
Thanks for the comments.
Bald36:
I would say it depends on how you define “strip scars”. I would say the average strip scar industry wide is not as good as this so no, “strip scars” are usually not this good. However not all clinics and surgeons are created equal and I believe doctors Hasson and Wong are as skilled as any at strip removal and closure. Over the last 15 years I’ve worked at the clinic I have seen many patients who have had their first strip surgery at another clinic before having one at Hasson and Wong. I would say at best one in every ten I would see would even come close to this one.
Dr. Hasson weighs in on your Question: “At Hasson and Wong we have always gone to great lengths to ensure our strip closures are as close to perfect as possible. So this patient has what we would consider a good Scar and probably 50% of our patients would achieve this or something close. The healing characteristics of patients do however vary but we would say 90% of our patients achieved scars of 2 millimeters or less.”
Here are more examples of well healed strip scars from our clinic:
https://hassonandwong.com/hair-transplant-surgery/hair-transplant-scars/
As far as part 2 of your question, I don’t believe he has lost much if any hair in the crown since his first procedure. The first surgery was to restore the front and mid scalp and work back as far as possible. Some light crown coverage was also able to be achieved. While this served him very well for several years it was always his thought to add to the crown at some point. The timing as mentioned was right to achieve the added coverage and density to the crown on this 2nd procedure.
-
A professional Hasson & Wong Patient Advisor will be in the following locations for free hair restoration consultations.
Seattle June 1-17
Dallas June 11-12
San Francisco June 22,23,24
Calgary July 4-5
Toronto July 9-10
Book an appointment by calling 1.800.859.2266 FREE or emailing us at info@hassonandwong.com
-
This was the original write up from a previous post back in 2014:
“This patient from Vancouver had been thinking of hair restoration for some time. The goal was to try for 4,000 grafts to restore the frontal zone working into the mid scalp as far back as possible.
He loosened his scalp for 2 months prior to surgery and Dr. Hasson was able to harvest 4435 follicular units in one session. 694 were single hair grafts, 3023 were doubles and 713 were 3 to 4 hair grafts.
The donor area was medium to high density and the caliber of the hair was fine. Dr. Hasson also was able to provide coverage in the crown while still delivering the adequate density up front. The patient was very grateful and pleased with the result which, especially considering his fine, hair worked out quite well.
These photos were taken a little over 3 years post-op.”








The light coverage in the crown as a result of his first procedure served him well over the years but now having some time off he decided he would like added density to that area. The combination of his scalp being tight, the previous scar being so good and the thought of having a quicker recovery all factored in to his decision to have FUE for his second smaller procedure. Considering all factors, I believe his decision to opt for FUE this time around was a good choice. As you can see in the pics, the scar from the first FUT procedure was very minimal, he can probably go almost as short as if he would have had FUE in the first surgery. Photos are pre-op, imed post op, 1 day po and 6 days po.
187 – s
1123 – d
683 - 3-4 hair
1993 total grafts
4482 hairs, manual, punch size 0.8








The following photos are 15 days post-op




I will update his future progress
-
Thanks for the comments and questions guys.
Diffused thinning over a large area can often pose greater challenges. Many factors can be involved when determining the best course of action. We were one of the first if not the first to shave the recipient area to successfully transplant in between existing hairs. This allows for a greater field of vision and the angle and direction of the native hair can be determined with a much higher rate of success then without shaving which is critical in preserving surrounding hairs. Shaving in my opinion is a critical first step in being able to transplant large numbers with high densities successfully among existing hairs. A surgeon is able to transplant among existing hairs without the shave in some cases but this generally is reserved for smaller cases and where less density is acceptable. But you still run a higher risk of some transection. The skill of the surgeon and his technique are also factors of course. For a case such as this, Dr. Hasson would have determined that he could successfully transplant in between native hair with little or no material damage to them. If he felt there was too much risk, he would not perform the surgery. This would likely be the case if this patient had come to see him years earlier and the overall potential cosmetic result would have not warranted the risk of surgery. In other words, he would have had too much hair, the loss was not that noticeable, some damage to native hair would be likely and surgery was not going to make a worthwhile difference in his appearance. In this case the hair loss was far enough along to warrant surgery and safely navigating between the existing hairs was determined to be a safe bet. As far as whether medication would have been recommended before surgery, in some cases, yes. In this case, we know that the patient has an above average donor supply of above average quality. We know that while he may recover some hair in the top and crown on medication alone, he is not likely to recover enough or any significant amount of hair in the front to make him happy and give him the styling options he desires. In some cases we would just do to the front and top, maybe 4,000-4,500 grafts and leave the crown to medication. Factors such as donor reserves, final hair loss pattern, the patient’s desires and goals all play a role in determining the best approach. When a patient has these donor reserves, he can have just about anything he wants within reason. For this patient, money was not a factor, he wanted the most hair he could get, he choose not to see how well the medication might respond to his crown and was excited about the prospect of getting maximum coverage and density in one session. If he could improve some of the native hair on the medication that would be icing on the cake but maintaining his existing hair was the reasonable goal. I suspected that any of his native hair that fell as a result of temporary shock loss starting growing back at the same time as the transplanted hair. I have reached out to him to help answer a few specific questions. He has been on medication for about 14 months and has not noticed any improvement of the native hair, maybe stable at best. He reports the shocked native hairs grew back rapidly but it was not until around 6 months post op that he felt very confident without a hat. He was worried during the shock loss period but reports that everything Dr. Hasson said would happen did, including that he would have a great head of hair. He may try and post here with further information when he gets a chance as he is presently traveling.
-
Transhair,
Over the years I have seen many cases similar to this where growth at the 4 month mark is very good and a considerable cosmetic improvement is already taking place. However, the average patient generally may not reach this level of growth until the 5 to 5.5 month mark.
-
This patient in his late 30's came from Australia to get as many grafts as possible. The aim was for 6,000 plus and we ended up with closer to 8,000. The area of need depicted in the photos at first glance does not look as extensive but the generalized thinning encompassed the entire top, front to back. Only finer miniaturized hairs were giving the illusion of coverage. This is more evident in the some of the progression pics. He was not able to style the hair properly and sun exposure to the top was always a concern down under. He had 3318 singles, 4170 doubles and 374 3-4 hair grafts. The quality and quantity of his donor hair was good. Medium to coarse in texture. He has an estimated 5,000 grafts left in reserve. The first 3 photos were taken at the clinic, the rest were sent in by the patient.












-
Dutchie,
It has been a pleasure to have you as a patient and we look forward to seeing you again should you decide on round two next year. You are in good hands either way, FUT or FUE.
The hair gods may be smiling on you but give yourself credit for doing your research, you helped make their job a lot easier:)
HTsoon/Spidey,
The transection rate on this patient in particular was very low. If I recall from the chart the percentage of what was planted versus what was extracted was high 90's%. I'm out of the clinic this week but when I return I'll see about getting the number.
-
Dutchie!
I hope all is well. I plan to update this every few months and hope to have the 1 year update as well.
HairLostyears:
He has high expectations so it wouldn’t surprise me if he considered round 2. But I have told him to wait for the full result.
For this case if we assume a total of 7,000 grafts, the patient would have very nice coverage and density and would essentially be done. If he continues to take Proscar he would not likely ever need another procedure. If he had FUT and 7,000, we can assume the result would be virtually the same. The only major differences would be with FUT he would have in theory another 3,000 or more grafts in the bank. With FUE he would be about tapped out. The factors such as medication, the scar, styling options, costs would all be considered. You can make a case for either method here.
Graft survival with our FUE technology is quite high, rivaling our strip survival. For this patient in particular, I didn’t see any drop off with regards to what his yield would have been with FUT.
You don’t need to call this a watershed moment but I would feel comfortable describing it as such.
delancy:
For the sake of this discussion let’s assume 7,000 grafts total in the donor reserves to start instead of 7377. If we assume the total number of grafts in the sides and back is 14,000 of which 7,000 can be used before it starts to look too thin, 7,000 would be left to create the normal appearance; we can then say his reserves represent 50% of the total grafts if I understand the question correctly.
-
HairLostYears,
The powers that be suggest up to around 3,000 grafts left in the donor bank via FUE.
-
Thanks for the comments guys!
mosd, the breakdown:
Singles: 531
Doubles: 1887
3’s: 1893
4's: 66
-
This patient in his 30's from Vancouver wanted maximum coverage via FUE. He had a total of 4377 grafts over 2 days. He was wearing his hair very short on his last visit and I encouraged him to let it grow a little longer. It is still quite short in these photos. I believe with a little more length it would have been even more impressive at this stage. I'll up date hopefully again with his 6.5-7 month pics.





-
Hi Guys, thanks for the comments. Yes he is thrilled and the transformation has been life changing as you can imagine. You can read his story in the blog section of our website.
RadioRunner: We do occasionally post scar pics but in virtually all cases the scar is not the focal point. This patient had previous scarring from his first procedure at the other clinic. Dr. Hasson did remove some of his old scar and also went above with a new scar to take as many grafts as possible. The sides were previously untouched so the scar in the photo is the result of the last two surgeries in an area exclusively harvested by Dr. Hasson.
densedream: Due in part to the high placement of the previous work, Dr. Hasson was able to transplant in and around the old grafts and completely camouflage without having to remove any of them. While not pretty on their own, the old work does provide some value as far as adding density to the "hidden" areas of the frontal zone.

-
future-ht,
I meant to get back to you on your question sooner. Yes, Dr. Hasson usually does a higher density in the frontal zone than in the mid scalp and crown. He feels the front has to have a certain density to look natural and provide the best result. All things otherwise being equal, a patient with 4,000 grafts placed in the frontal zone and mid scalp will likely have the same density in the frontal zone than a patient with 5,500 grafts placed in the frontal, mid and crown. Both may have approximately 3,000 grafts placed in the front 1/3 of the scalp. Once the frontal zone is reconstructed, the number of grafts he has to work with will dictate how much density and coverage can be achieved behind the frontal zone.
-
voxman,
You're correct, no regrets. The scar was a non issue as is the case in our experience with most of our patients. He could not find the scar and didn't pay any attention to it. He could proably go quite short in the back but what are the chances ?


-
This musician from Calgary came to visit us based on a recommendation from an acquaintance. Dr. Hasson was able to harvest 5761 grafts to address his extensive hair loss in one session. He had 1344 single hair grafts, 4024 doubles and 393 3-4 hair units. Strip size was 30cm x 1.5-2cm. Above average donor hair with average hair caliber. He started topical Finasteride at the time of surgery. These photos sent in by the patient were 8 months post-op. As you can imagine he is very pleased so far with the result and this bass player/singer once again looks the part. He will be making a trip out to Vancouver this summer where we plan to take photos and video. We will update his case in the coming months.


-
fortune11, you hit the nail on the head. When this patient walked back in the clinic 1 year post-op I had to do a double take. I thought I'd hopped in the DeLorean back to 1983 and saw Jerry Reed from Smokey and the Bandit walk through the door............

-
Here's a couple more shots

-
Thanks for all the comments, I agree, quite the transformation.
delancey: Dr. Hasson did indeed classify this patient as a NW6
-
Many prospective patients focus on the donor area scarring. Any type of surgery whether it be fut or fue will result in some degree of scarring in the donor area. While it is important to consider the impact the procedure will have on the donor region, often times too much emphasis is placed here and not enough on the final result and how the recipient area will look. Hasson and Wong perform countless repair surgeries every year so I've seen many bad strip scars as well as bad fue scarring from other clinics over the years. Just because it's fue doesn't mean there are no scars. In fact, the actual square centimeters of scar tissue is larger per graft in fue than in a typical strip scar from our clinic. For the sake of this discussion, we'll focus on donor area strip scarring and more specifically as it relates to our clinic. The two key components in achieving minimal scarring in the donor area are knowledge and skill of the surgeon and the individual patient's healing characteristics. When the two components are favorable, the result is a fine liner scar. If a patient has very good healing characteristics but the surgeon had done a poor job of removal and closure, the resulting scar can be less than desirable. If the patient heals poorly and the surgeon is highly skilled, the resulting scar can be less than ideal but likley much better than in the first scenario.In most cases, the surgeons role can have the greatest impact. Below is a link to a video we've put together showing strip scars from Hasson and Wong patients. These are patients with good healing characteristics. One other thing to consider is that the size of the surgery and width of the strip has no bearing on the resulting scar if done properly. Many incorrectly assume the bigger the surgery size the bigger the scar, not so. You'll see the 8400 graft 1 session result has virtually no visible scar. Keep in mind these are Hasson and Wong patients and not all surgeons are created equal.
Dr. Hasson 3252 FUT one session/ gel, 7 months post-op
in Results Posted by Leading Hair Restoration Clinics
Posted
Vancouver patient in his mid-30’s with medium/coarse hair. Dr. Hasson and team transplanted 3252 grafts in one session comprised of 1198 single hair grafts, 1889 doubles and 165 multi hair grafts.
These photos were taken 7 months post-op at the clinic and the patient had gel in his hair.
At 7 months things are looking quite good. Dr. Hasson he ran into him months later and said he looked "unbelievable". I hope to get him in for updated pics.
right:
left: