

Janna
-
Posts
2,041 -
Joined
-
Last visited
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by Janna
-
-
-
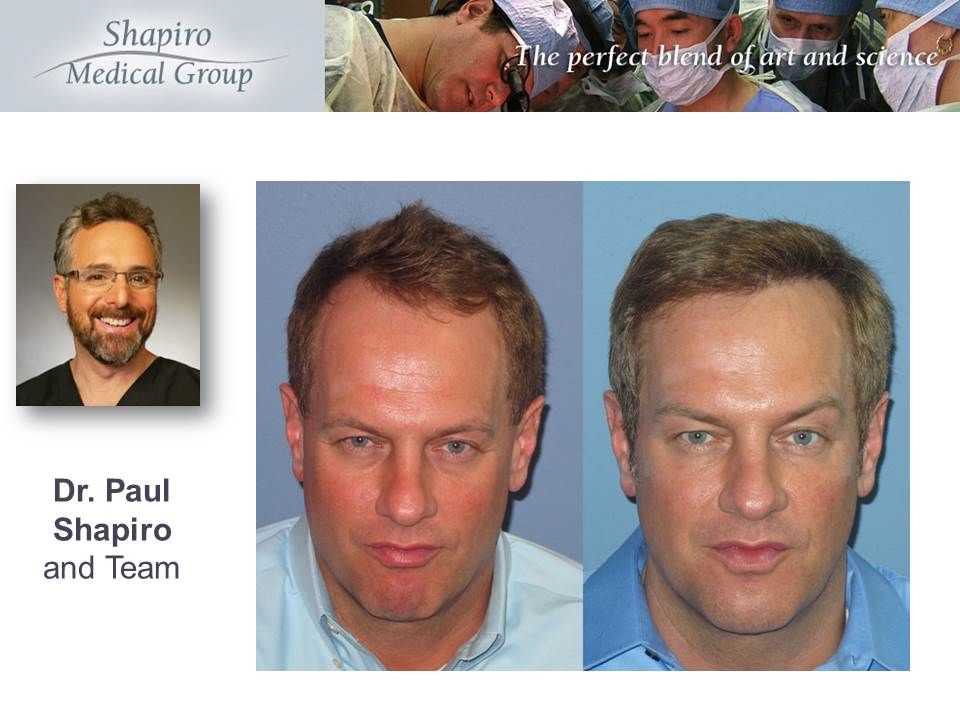
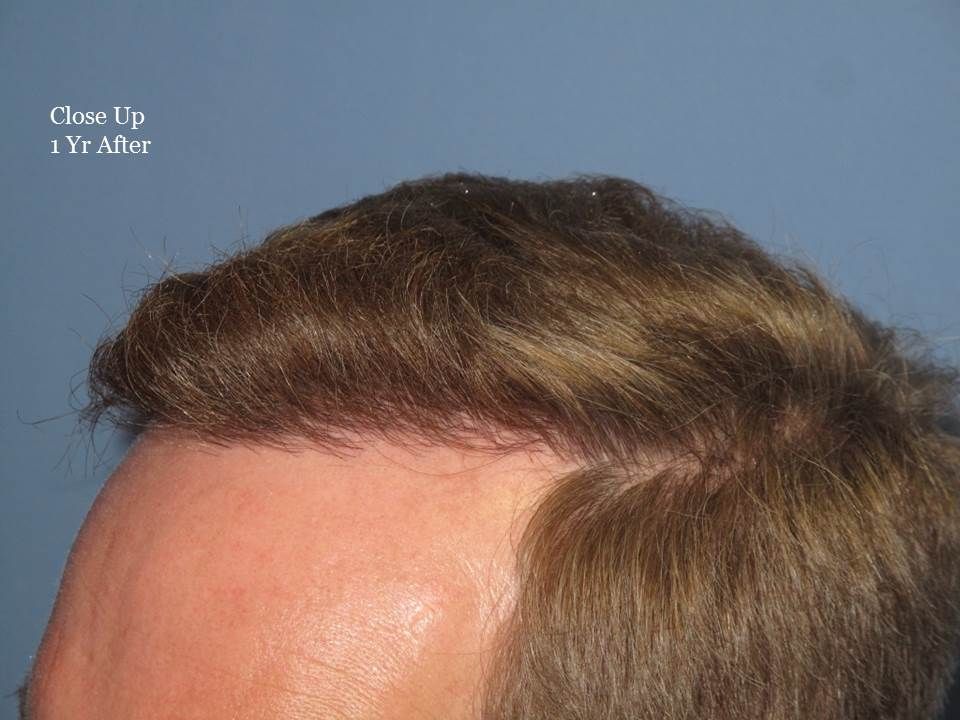
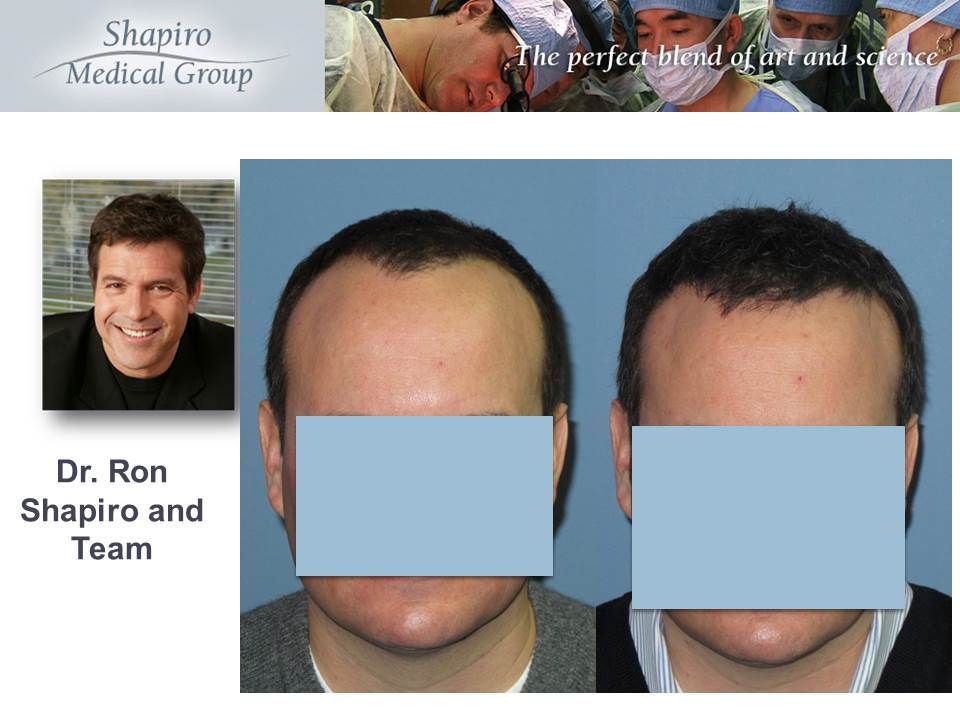
I agree he's lucky to have almost a full head of hair in his late 40's.
Thanks for the feedback.
-
You're making great progress. You have another 6-8 months of growth/thickening to look forward to. I agree that you have contributed greatly to this forum and I'm happy for you on the type result you're achieving. As for the pics you've posted - I think it's a bit unfair for any to state your pics are the worst. I've seen much worse and some have been from clinics too.
I know you've been debating about thickeners like Cobuki and Nanogen. DermMatch, Toppiks, etc are all very effective. You have to be careful to not use too much but I definately don't see any shame in utilizing them.
-
-
Thank you for your feedback!
 :)
:) -
-
-
We have all our strip procedure patients apply the antibiotic cream Bacitracin right after their daily shampoo for the first 5 days. We've been doing this technique for years as we feel it's been beneficial in producing better scars.
-
We encourage all our patients who are concerned with growth to contact us directly so that we can assess their progress properly.
We have a reputation for being conservative and cautious and it's especially true with the Artas. We feel it's better to be cautious than be agressive with a new instrumentation. So the issue of growth may be due to less grafts rather than the extraction method.
As mentioned below of Dr. Ron's participation in the Artas conference in February, I encourage those with issues and concerns to meet with him in Southern California next week.
I recently addressed some of the concerns with the Artas on another thread - here is my post:
-----------------------------------------------------------------------------------------
We understand that there are some issues of growth/concerns with few of our patients who had the Artas used.
No matter what type of procedure we do at SMG, we take utmost care in achieving satifactory outcomes . Please contact Matt or myself so that our physicians can review your files objectively with proper pictures and surgery data. If there is an issue of yield with the Artas, we'd certainly like to know about it. Aside from few posters here, the feedback we've been getting from our Artas patients have been positive. There is a conference next week with Restoration Robotics and all the physicians using the ARTAS, it'd be good to present our cases whether it's positive or negative.
When we first started using the Artas, the main concern we were hearing was the size of the punch, that the dull punch size was considered too big and therefore it may create unexceptable donor scars. We started and still maintain our cautious approach in using the Artas. We generally start off the two day FUE procedure by using the Artas the first day. If the grafts look good under the microscope we'd proceed, or switch to SAFE if the extractions were difficult. The second day we'd use the SAFE method to even out the extraction pattern and get remaining grafts needed.
-
Hi,
We understand that there are some issues of growth/concerns with few of our patients who had the Artas used.
No matter what type of procedure we do at SMG, we take utmost care in achieving satifactory outcomes . Please contact Matt or myself so that our physicians can review your files objectively with proper pictures and surgery data. If there is an issue of yield with the Artas, we'd certainly like to know about it. Aside from few posters here, the feedback we've been getting from our Artas patients have been positive. There is a conference next week with Restoration Robotics and all the physicians using the ARTAS, it'd be good to present our cases whether it's positive or negative.
When we first started using the Artas, the main concern we were hearing was the size of the punch, that the dull punch size was considered too big and therefore it may create unexceptable donor scars. We started and still maintain our cautious approach in using the Artas. We generally start off the two day FUE procedure by using the Artas the first day. If the grafts look good under the microscope we'd proceed, or switch to SAFE if the extractions were difficult. The second day we'd use the SAFE method to even out the extraction pattern and get remaining grafts needed.
-
We typically like to check up on ht surgery progress at 6 and 12 months, however, Matt at SMG always likes to see patients for their first check up at 7 mos rather than at 6 mos. He feels the one extra month between 6 & 7 makes a world of difference. Great to hear you're getting nice growth this early on.
-
-
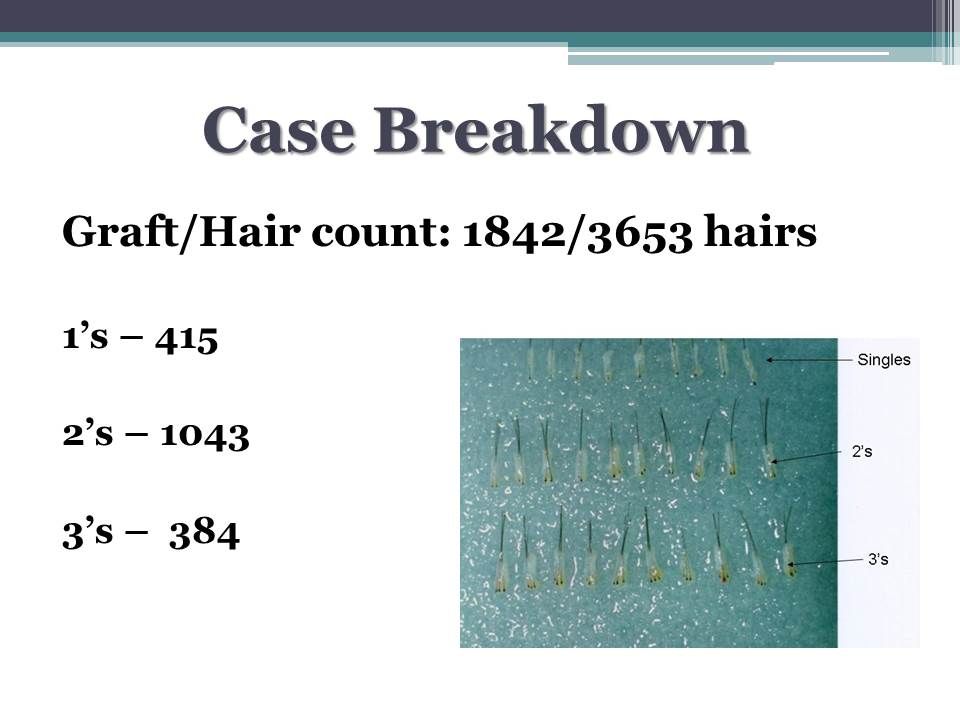
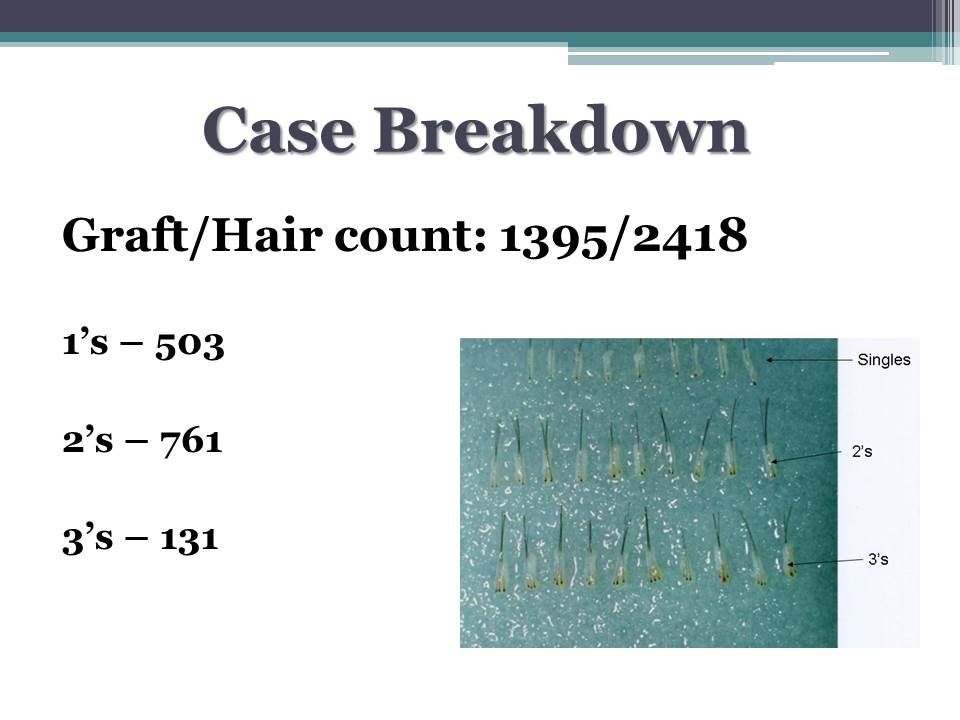
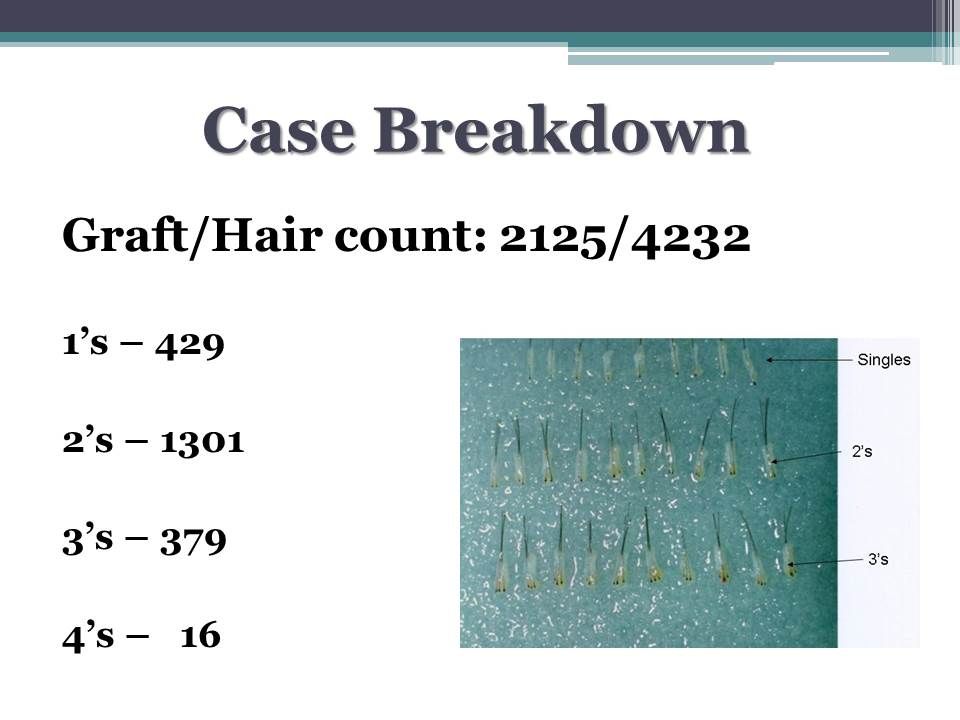
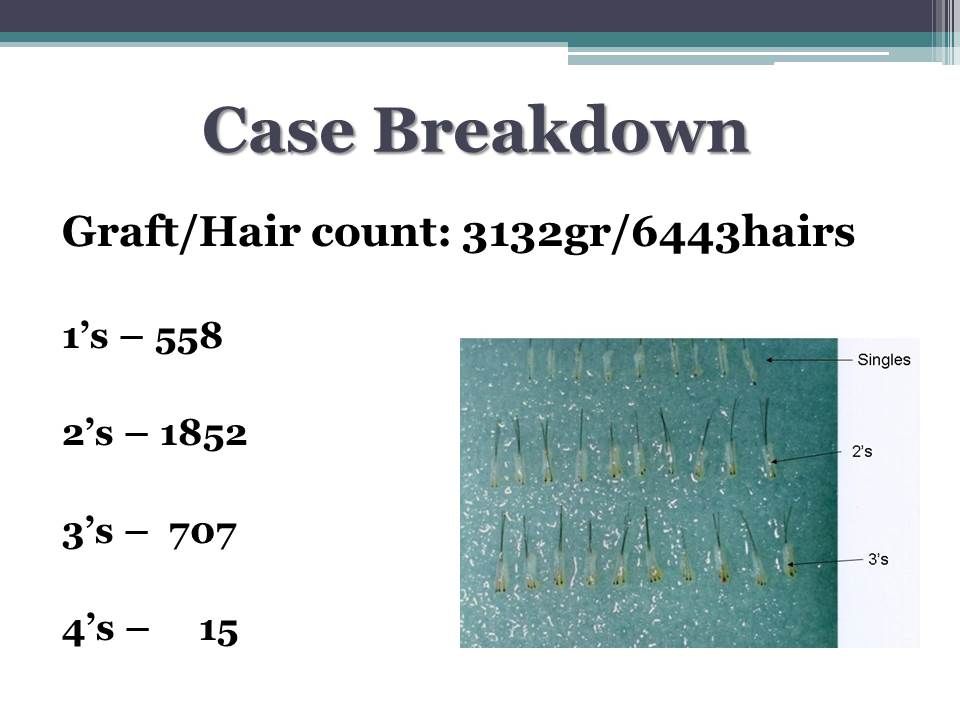
It depends on the size of the slits made for each incision. The bigger incisions can hold multiple grafts. Did you ask about the disparity in the #of incisons versus the # of grafts?
-
It's likely you can use some limited Toppiks since you're 3 weeks post op, however, you should check with your ht physician as to when they feel comfortable with their patients using filler-products.
It's normal to "shed" your transplanted hairs. Expect to shed majority of the transplanted hairs in the first 2 months. If some of your native hairs fell out due to shock, they should return in approximately 3 months.
-
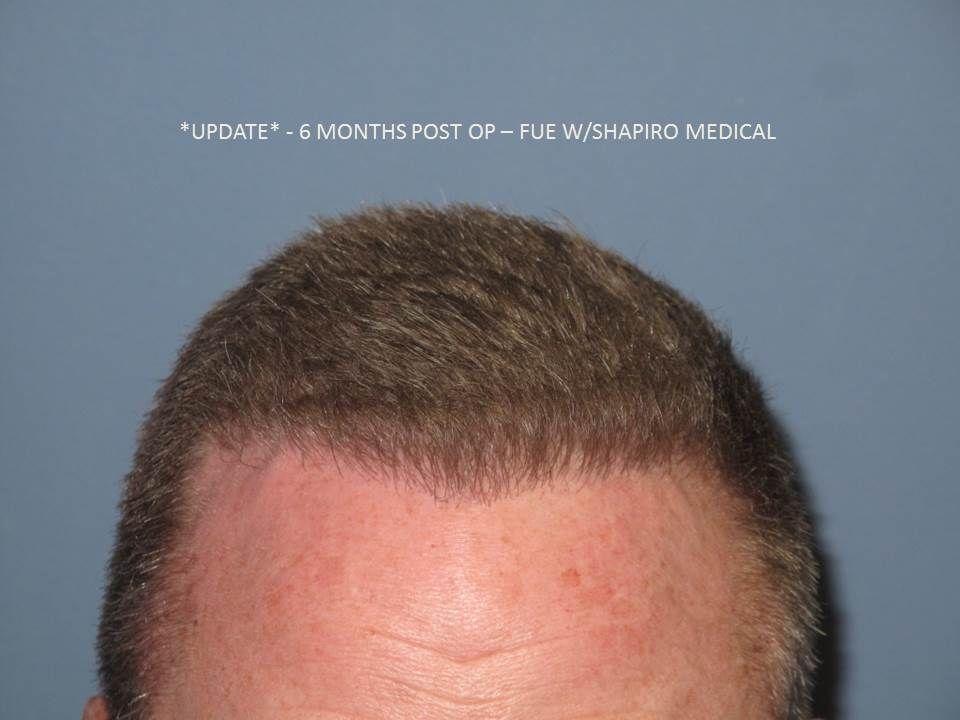
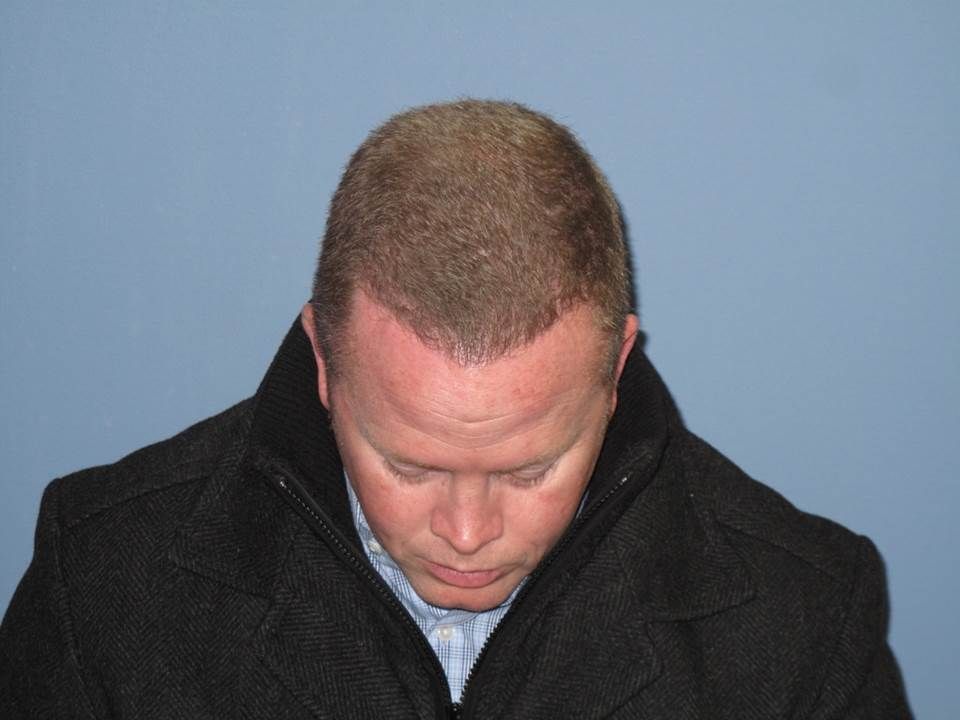
There's been a nice improvement from month 5 to 6 -








-
However, all things being equal, I find that the tools are becoming less of an issue as each practitioner of hair restoration will find the best tool that suits their practice. Just because someone has a procedure with lateral slits does not mean that the result will be obviously better than his identical twin that had a procedure with needles or an implanter pen from a different doctor. I really like Dr. Lorenzo and I respect his work with the implanter. He has great results. Same goes for several other doctors that use needles such as Rahal and Shapiro.
In the end, it comes down to finding a doctor that is comfortable with his tool of choice but more importantly is showing consistency with his work, day in and day out. If you find a doctor that has a deep library of results that makes you say "wow" regardless of technique or tools then that is all that really matters as long as the results are being presented in an honest and transparent fashion.
I agree with Joe on what's he's said above but I'd like to make a small correction that physicians at Shapiro Medical do not use needles to make incisions. We use custom cut blades but we typically use a combination of saggital and coronal incisions.
We've tried needles and various implanters but they did not suit us. With the implanter there will be times when implanting the surrounding grafts will pop out partially or all the way depending on the individual patient. It's not to say you don't encounter bleeding or popping issues with lateral or saggital incisions as well. The clinics who have trained and experienced technicians for planting properly will not likely use implanters. Implanters don't necessarily speed up the surgery time. I've mentioned before that I've visited Dr. Lorenso's clinic and that he's one of the hardest working physicians around because at the time of my visit he said he routinely works past 8-9pm. The night before my arrival he said he worked till midnight. The traditional way of planting with fine forceps can utilize up to 3 planters at once.
As Joe said above, producing consistent results in the right hands regardless of the tools is what matters. As we all know, poor results have been achieved when best tools were used.
-
You can add Shapiro Medical Group to your list.
We've been using the ATP post op spray and so far we're encourage by what we see on our patients. The redness from surgery is almost gone within a few days. Amazing what the recipient area looks like even the next day. We've used graftcyte post op spray prior to ATP spray and we were always satisfied but ATP spray brings the post op healing to another level.
-
If the follicle stays intact under the skin, then no, that follicle with hair pulled out or not should produce new hair in due time.
I'd caution, however, to NOT take the tweezers and pull the hairs from a newly transplanted graft. What senario would a patient need to pull the transplanted hairs out? The only time it'd be recommended it if you saw a transplanted hair that basically stalled - this means that the transplanted hair never shed within the first 2 months after surgery and just continued to linger on for months after. I've suggested to some patients to gently pull these out. They come out with any resistence. A new hair will grow in it's place shortly after.
-
Very nice result!!
-
Beautiful eyebrow result!! Eyebrow work is more difficult than most patient believe it to be.
-
It's interesting how so many people want to address the crown first. You will find that most (if not all) surgeons recommend you take care of the frontal third/hairline first because it frames your face and that is what people notice first. Also, you have limited donor supply (everyone does), so you don't want to exhaust grafts on something most people don't notice right away. The meds should help stabilize the hair loss in the crown area and thicken it up a bit. I'd try that for 12 months and in the meantime research hair restoration and learn everything you can about it. You'll have a different perspective then and go into it well-informed.
Well said by Since21 and I echo pretty much the same info here.
There are so many patients who have uneven hairloss pattern that you're definitely not alone.
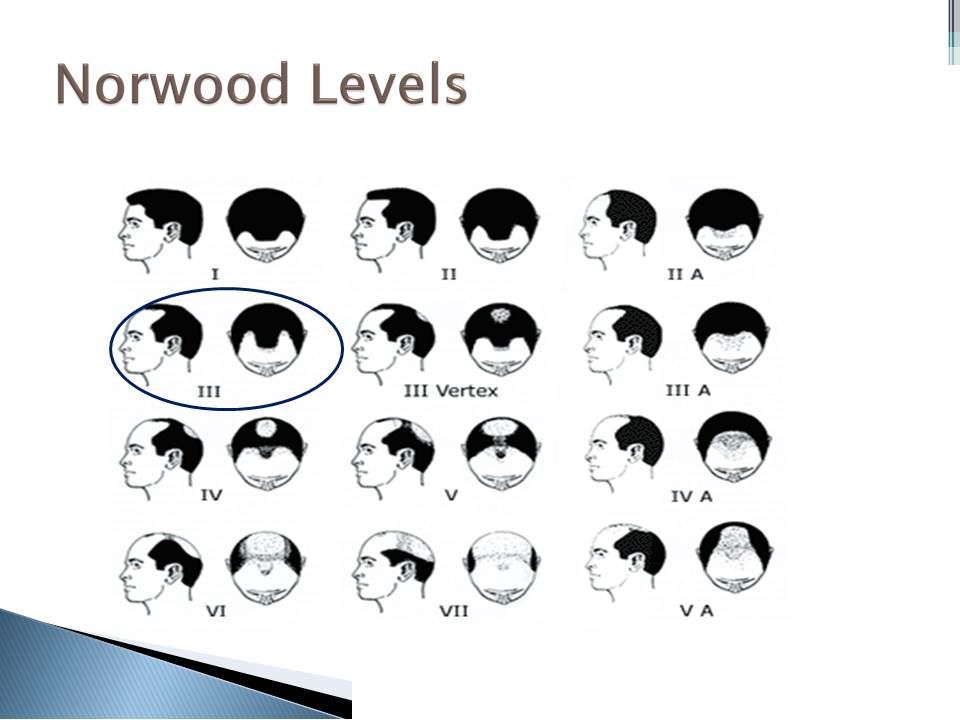
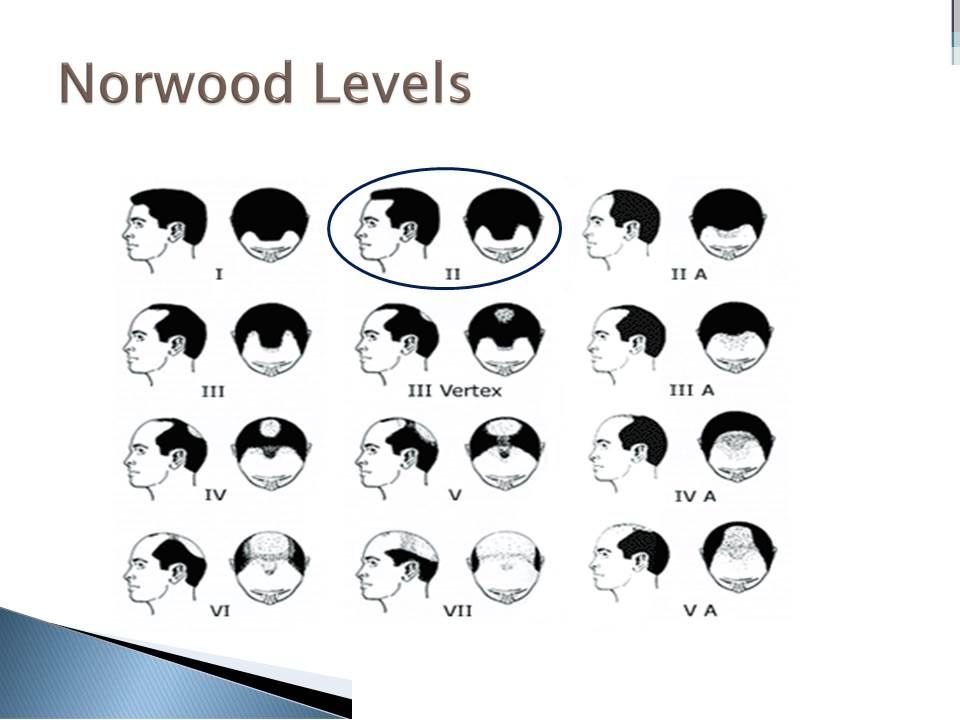
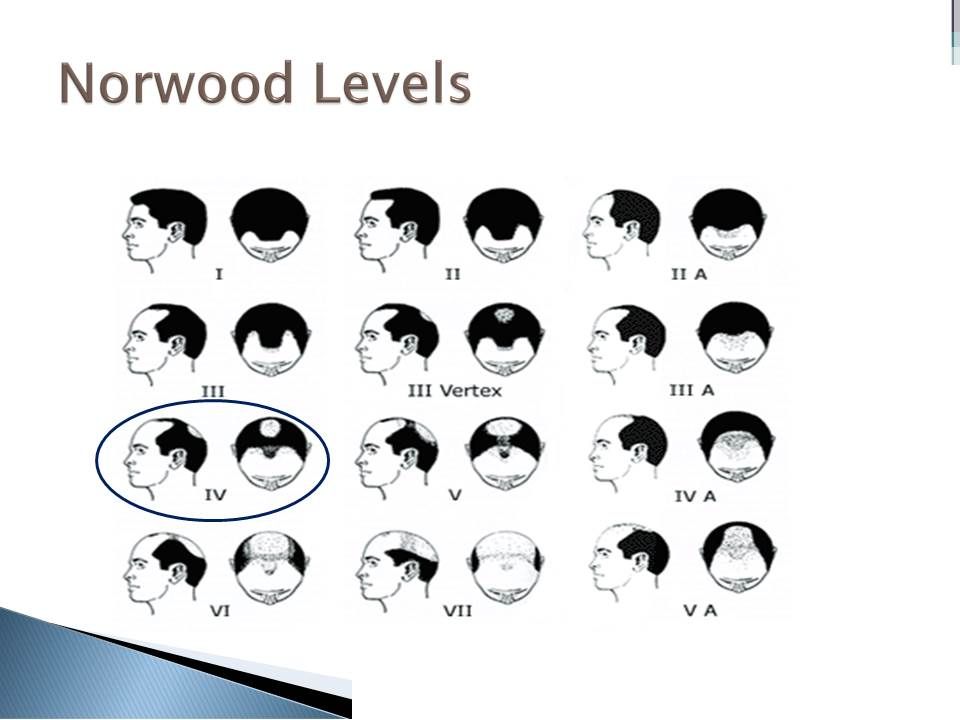
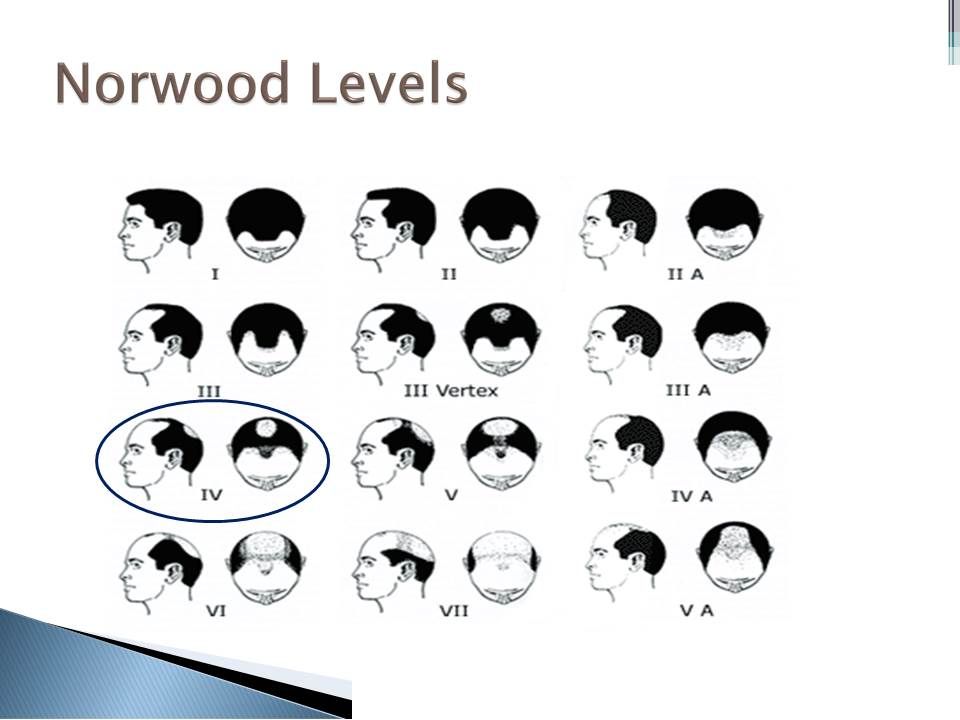
Do try to stablize your hair loss first so the limited donor supply can be utilized in the best manner. You can address your crown in the future if your hair loss hasn't progressed much. Since no one knows what Norwood level you'll end up it's better to address the areas that bother you the most, which is usually the top half. The most effective way to stabilize your loss is through Finastride and Rogaine foam. If meds are not something you're willing to do then how you address your loss with hair surgery becomes even more important.
-
What you do with a graft at day 3 to day 10 can have vastly different outcome. I don't understand your questions. How are you able to remove a hair at post op day #3 without removing the follicle too?
-
-
We used to tell our patients to apply Rogaine a week after surgery, however, we notice there were many patients stating they were experiencing some form of skin irritation so soon after surgery. We now ask them to start applying on the recipient area 2 weeks after surgery. It's best to start off gradually to test your skin condition. If all is fine after few days, then apply normally.


























Propecia or Biotin?
in Hair Restoration Questions and Answers
Posted
Biotin doesn't have the track record of retaining or possibly regrowing lost hairs like Propecia. Use the Minox and Propecia at the same time - it'll give you the best result. There's nothing wrong with continuing with Biotin while on Propecia and Minox at the same time.