

Dr. Carlos Wesley
-
Posts
682 -
Joined
-
Last visited
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by Dr. Carlos Wesley
-
-
-
The piloscope is now ready for limited clinical use in a select group of patients. Development and testing of the device that enables select harvesting of the stem-cell containing portion of hair follicles without traumatizing the overlying skin surface has led us to this point. The company (Pilofocus) overview can be seen here.
Beginning at the end of July 2015, a handful of patients will be able to undergo very limited surgical hair restoration with this method. The cases will initially involve transplantation of approximately 100-200 follicular units. Although this "scarless surgical" method will eventually be made available to all hair types, patients most suitable for the initial piloscopic procedures are those who have previously undergone follicular unit transplantation (FUT) as the instrument will harvest donor hair adjacent to their donor scar. There is no charge for patients selected to take part in these initial, small pilosocpic procedures.
Please email, Barbara, our office manager at info@drcarloswesley.com or call 844-PILOFOCUS (1-844-745-6362) for more information.
-
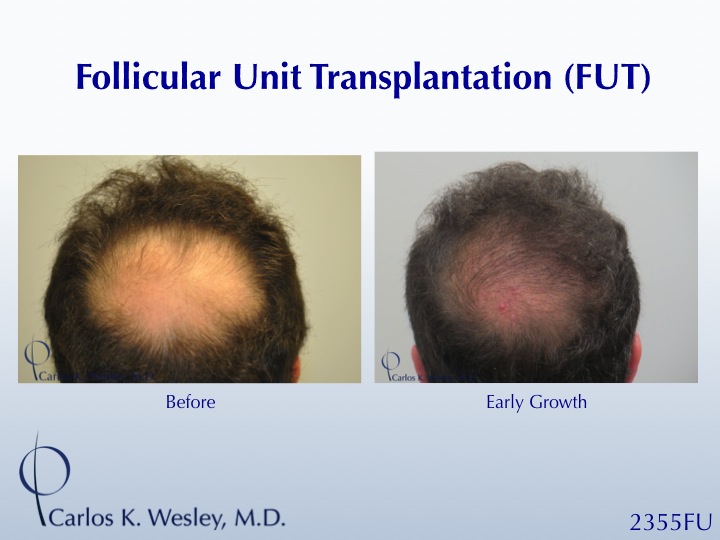
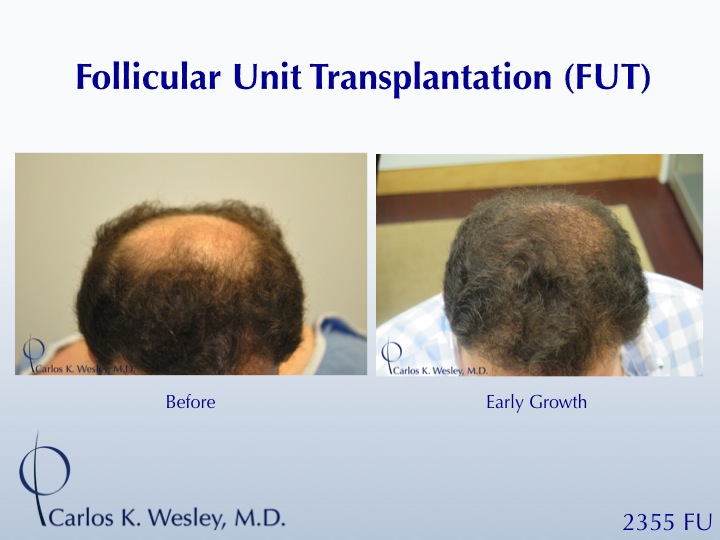
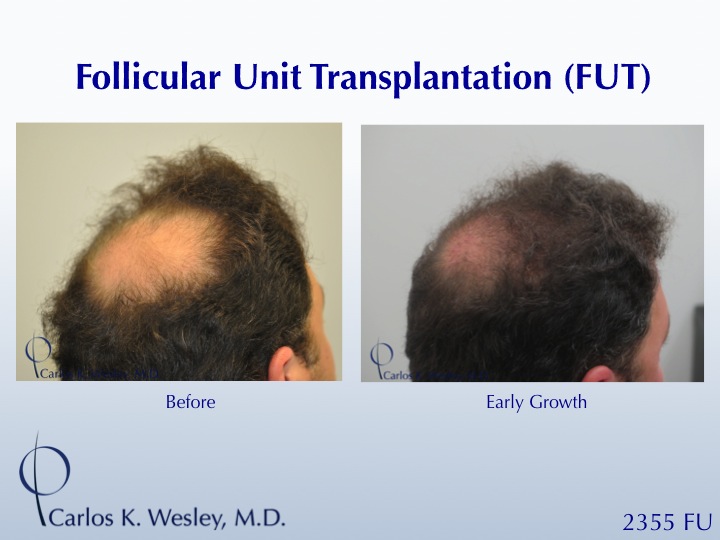
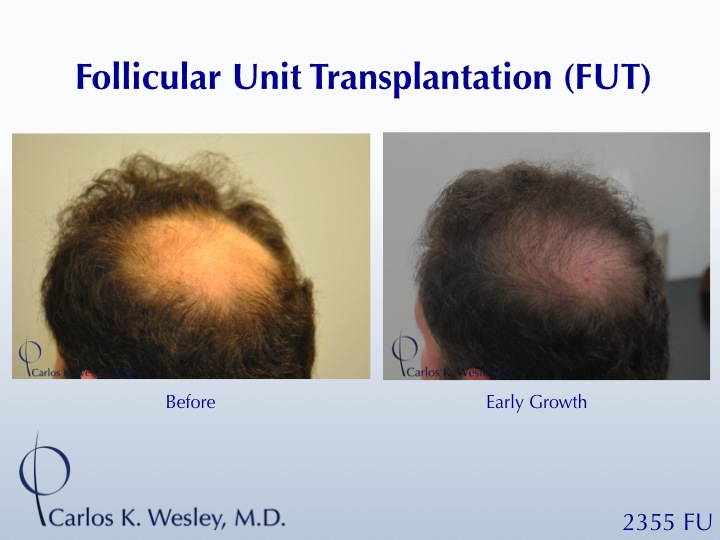
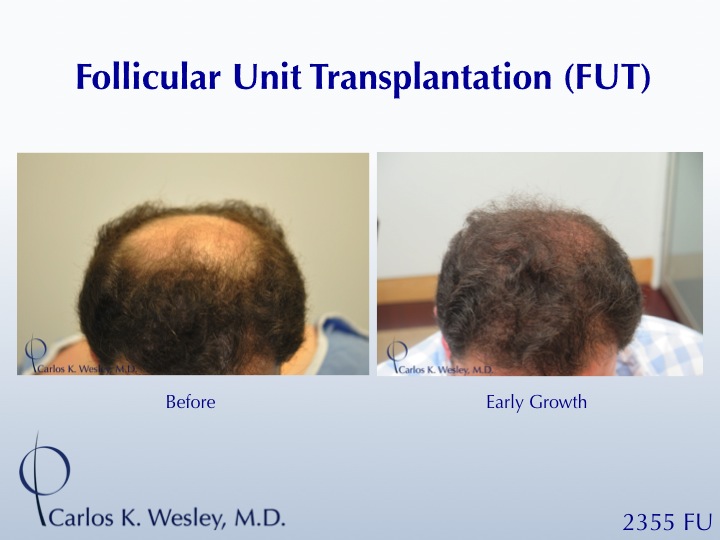
We appreciate your comments. I'm especially glad to hear that so many of you are able to understand the benefit of not only addressing the "now" (the 30s, in this patient's case), but also planning for later in life when more severe hair loss surrounding an isolated transplanted region would start to look unnatural and draw attention to itself.
Often times, as demonstrated in this patient scenario, increasing hair fullness within a hairline gives the illusion of lowering a hairline without actually lowering it. The patient loves this in the short term because the fuller hairline provides a healthier facial framing. It's equally important as well that the patient is appreciative down the road when they maintain an age-appropriate hairline that still looks natural.
-
Thanks, all, for your kind words. Although I cannot speak for every hair restoration specialist, it is standard operating procedure in our practice to use a combination of PRP and ACell as a storage solution for follicular units when they are out of the body in both our FUE and FUT cases.
The upside: It has been demonstrated to generate a statistically significant improvement in survival and caliber (thickness) of transplanted hair follicles. I've also found the hair growth to occur earlier and the redness to be minimized.
The downside: It demands a large, dedicated staff as the process requires a staff member to focus on the isolation and creation of the PRP as the surgical procedure is taking place.
-
Thanks for your comments. The donor scar extended along half of this patient's donor area (occiput, parietal, & temporal regions). It's just nice for patients to know that this option exists as knowing that it can be well camouflaged often allays concerns regarding long-term donor scaring from FUT.
-
Thanks, hair there!
Another nice aspect of the PRP/ACell augmentation of density is that it can be re-administered years after the procedure as desired. Our office was glad to see that this treatment for hair loss in women was highlighted in a recent NYTimes article (below)

-
Many patients have inquired about the current status of development for the piloscopic surgical technique. Therefore, I wanted to share a link from my recent presentation delivered at the 2015 American Academy of Cosmetic Surgery Meeting that provides both an overview and an update. I hope that you find this helpful.
-
This patient desired more fullness in his eyebrows. Using a 0.8mm FUE punch, a combination of body hair (leg) and scalp hair from the temporal region was used to treat both eyebrows. The patient returned to our NYC surgical clinic 11 months after his session to display his results. Grafts were incubated in PRP and ACell throughout the procedure.




-
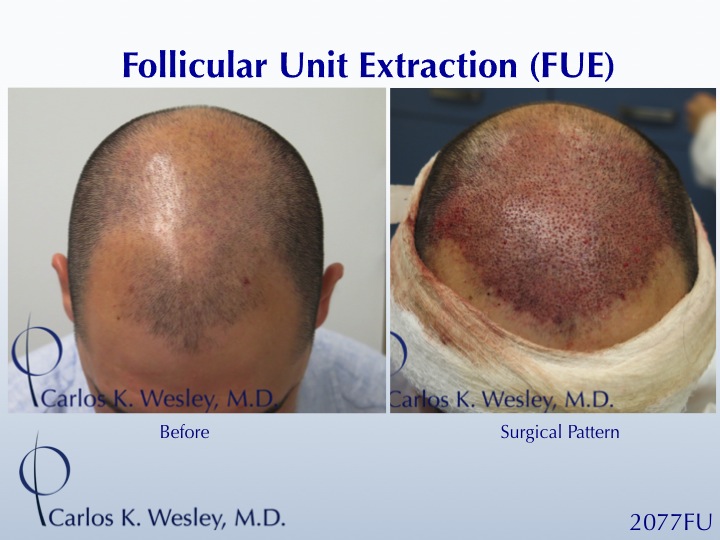
Thanks for your comments (and unanticipated controversy!). Yes. I can attest that this is the same patient in all images. As our office couples before and after images together, we occasionally use the same "before" pic with a different "after" pic to achieve a different pairing for comparison. I think this helps give a better sense of the result. The "blonde" look of the hair was simply due to the reflection from the OR light above. If it helps, our office will post a video of this patient shortly. Meanwhile, I have attached intra-operative pics of my pattern and density of FUE transplantation.


-
Thanks again for your comments on this interesting subject. Your crane worker analogy, fisher4man, is certainly an interesting one! It's actually five days until transplanted hair follicles have established their own capillary network. The life of a platelet is 10 days. However, it's not necessarily the platelets, but rather their growth factors and cell recruitment that benefit the follicle during this vulnerable period. Although I agree that PRP/ACell therapy is by no means a guarantee, I have seen it show promise in the appropriate candidate (those with miniaturized hairs that are often surrounded by evidence of dried keratinocytes).
And, yes. The OR lighting may not have been exactly the same. We therefore included the magnified timeline images in the video to demonstrate the true progression of hair growth in the male patient.
Thanks, ontop, for your comment. The female patient will likely return for a repeat injection at the 7 month mark after her first. Studies on PRP injections have demonstrated that it's roughly at the 7th month when hair caliber and growth peak from an initial injection. After that time period, we'll continue to monitor her.
I've been asked to write about PRP in the "Future of HT" section of the upcoming "Hair Transplantation" text book. To illustrate how much uncertainly is surrounding this therapy, at the 2013 ISHRS Meeting, a panel of five hair restoration specialists were asked to describe their PRP injection protocol. All five of them used different methods to isolated the PRP, all five had different concentrations of PRP, all five had different preferred intervals or treatment, and all five reported slightly different patient results.
Although it's a procedure with promise, there's a LOT yet to be determined (much like low level light therapy). The one thing I would say with certainty is that you should avoid PRP injections if the doctor tells you it's "guaranteed" and/or if they are suggesting it without first carefully examining the patient with a magnified camera to closely evaluate the scalp.
-
This woman has Hamilton type female pattern hair loss (FPHL). You're correct, fisher4man, in that it looks like traction alopecia. Many people can confuse the two. However, in this case, her Hamilton type AGA demonstrates bitemporal recessions and has a classical distribution of male pattern baldness - thinning evident in the lateral-frontal part of her scalp. These slowly-progessing thinning of recessions is often something we see in peri-menopausal female patients and a few scattered terminal hairs are often viewed within the numerous finer, miniaturized hairs. If you would like to read more about FPHL, here is a great article that describes it in more detail.
She is a very good candidate for surgery rather than simply injections because of the health (density and caliber) of her donor area. The PRP/ACell combination used to treat her grafts during her case simply helps ensure a healthy result. We have treated numerous patients as you mentioned - with unilateral injections (one side and not the other). However, (due to its systemic recruitment of cells) the effect of PRP/ACell is not focal, but rather more diffuse. So, unlike transplanting hair into an isolated square to measure its viability, the efficacy of PRP injections cannot simply be measured by adding it only to one portion of the scalp.
-
Thanks for the important (and somewhat controversial) topic. Platelet rich plasma (PRP) is a treatment that has certainly shown promise in our field of hair restoration. Probably the most important criteria in determining its beneficial effect is appropriate patient selection. The main challenge in presenting objective data worldwide is that there is so much variation regarding concentration used and technique of PRP creation and delivery. During last year's ISHRS meeting, five respected surgeons on a PRP panel all revealed that they use completely different techniques and methods of harvesting PRP.
Dr. Carlos Uebel in Brazil published quite a thorough study in 2006 in which he demonstrated the benefit of PRP as a storage solution during hair surgical procedures. We have found the same trends to be true: improved survival and hair caliber post transplantation.
As far as a stand-alone injection procedure, I will have our office manager post results tomorrow on this site. It can be incredibly effective in the correct patient. Our examination last year revealed that (although PRP's benefit is not gender specific) women often respond best. It is important to have proper evaluation prior to undergoing PRP. What I mean by this is patients with evidence of miniaturized hairs and/or dried perifollicular keratinocytes often respond well.
I've been asked to write about PRP in hair restoration in the upcoming Hair Transplantation textbook and will keep you all updated on the trends I find though out the world.
-
Thank you, David. This patient has been very pleased with his early growth and there is still plenty more to come.
-
Hi, KO. This patient had a follow-up procedure in which we covered the entire crown as well as areas of future loss. I'll be sure to have our office update images to demonstrate his complete coverage.
-
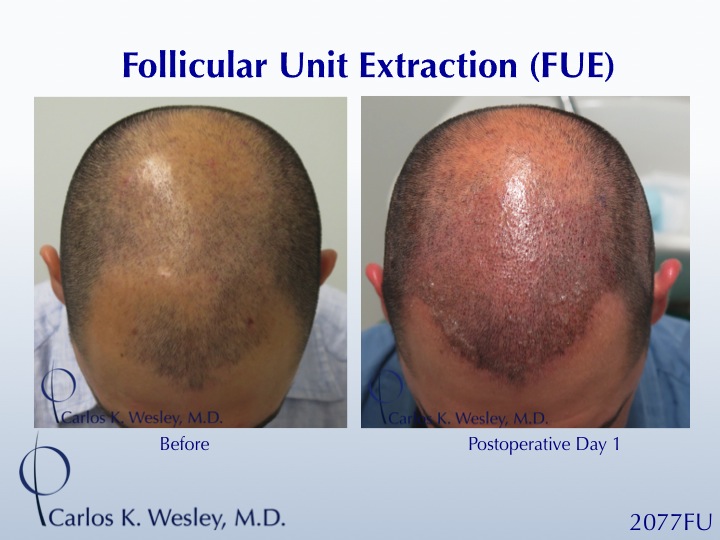
A common postoperative concern that my patients express is, "when can I safely shampoo my hair?" Our patients always return to our office the morning following their procedure. During this visit, we remove the protective bandage and perform the first hairwash. It also allows for any fine adjustment of follicle placement.
The answer to "when" often depends on the characteristics of the follicles during graft placement (i.e. if the grafts are "slippery" or if the placement of a neighboring graft alters the depth of a nearby graft). Perhaps one of the most important characteristics is follicle root depth.
The mean depth of a scalp hair follicle is 4.16mm. Our patients are generally able to gently wash their own scalp (including the grafts) on postoperative day 3 or 4. When we note particularly long grafts (as seen below), patients may safely perform a gentle shampoo slightly earlier (days 2 or 3).
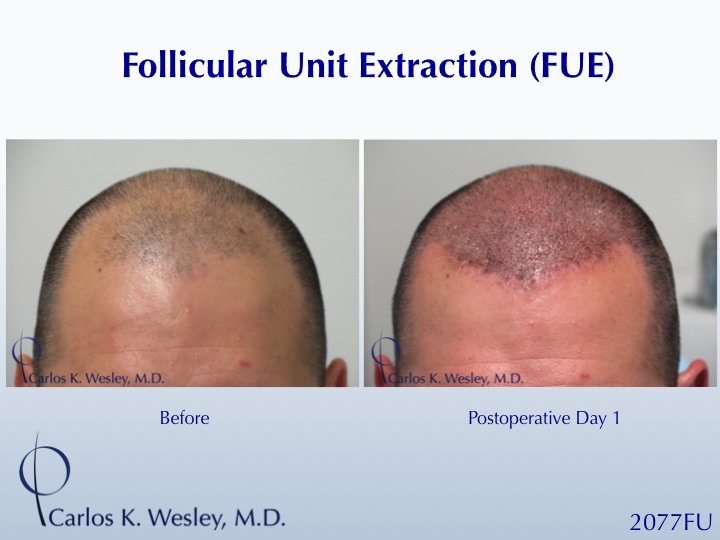
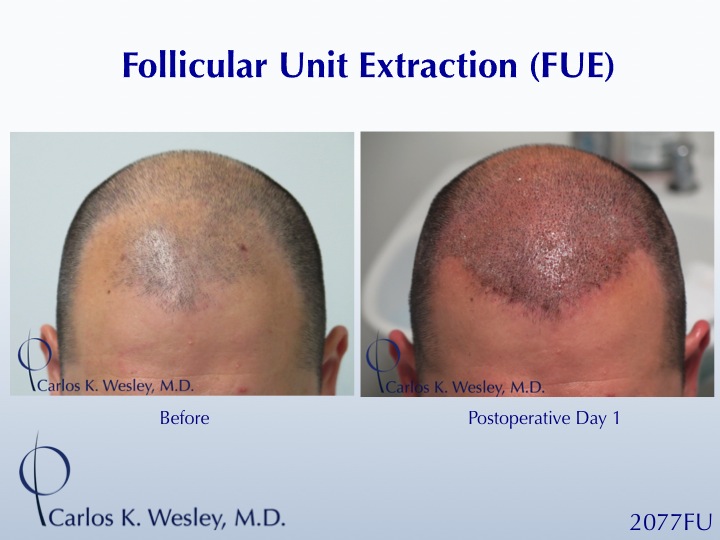
It is important to realize that these determinations are made by the physician performing the surgery as they are based on intraoperative findings. Fortunately, I believe all of the recommended physicians on this network are involved in all three phases of the procedure (pre-op, intra-op, and post-op). So, be sure to get your advice from them after the procedure.
This patient had grafts over 5mm in depth. His pattern is seen day one postoperatively. He was able to perform a gentle hairwash on day 3 as a result of his hair characteristics.

-
Forgive me for indulging, but I can't help but share the "hair tips" offered by my wife, Anna Kaiser, yesterday on Yahoo Beauty's article "How Top Fitness Instructors Maintain Such Great Hair".
Proud of her!
-
Fair question, KO. We had numerous discussions regarding FUE or FUT. Essentially, the density (via use of FFs) was most important in the patient's eyes as well as the importance of having more protective tissue around the stem cell-containing portion of each graft. I'll have our office post a video of his donor as it looks great and he can wear his hair at a very short length.
-
Thank you, Voxman. Perhaps now, with his new hairstyle, he'll consider running in 2016!
-
Thanks, Mickey85. The donor was a pretty important element of our pre-op conversations. He wanted to be sure that he could still get wear a short hair style. In his case, I'm not sure that this would have been possible without using a trichophytic closure.
-
A common observation amongst patients during the early phase of hair growth following surgical hair restoration (either FUT or FUE) is ingrown hair follicles. The "pimples" that some (but not all) patients experience generally represent focal inflammation (folliculitis) where a newly-ingrowing hairs are beginning to surface.
Patients can often feel reassured knowing that these generally precede more apparent hair growth over the following weeks and months. They can be seen in both the recipient area (where transplanted hairs are coming in) or donor region (especially in FUE where any residual hair fragments may be coming in). They may be more commonly observed in zones where the angle of hair implantation is the sharpest angle (e.g. the vertex or crown as seen in the attached image)
In general, a simple cotton ball soaked in rubbing alcohol can be used to rub on each pimple. The microabrasion allows the nearly-ingrowing hair to surface and resume growth. It's relatively rare that an antibiotic is required, but even a one-week course of antibiotic can have a positive impact. The ultimate appearance is not impacted by the presence absence of a few "pimples" and patients should simply be aware that they generally represent an early phase of growth.

-
Thanks, johnboy71 and hairthere. Much appreciated!
-
Thanks, Spanker, for your comment. He's very pleased!
-
Thanks for initiating this tread, crafter. Although not such an uncommon sentiment, syban's "DoomsDay" post might be a little premature. There's some good science out there already. In my opinion, it's a matter of taking those well-structured studies and applying them to our field in the way they'll benefit patients most. I just posted an article on Twitter. That was quite an undertaking! I haven't figured out how to share that link yet, but you're welcome to check it out there or simply type it into your URL.
-
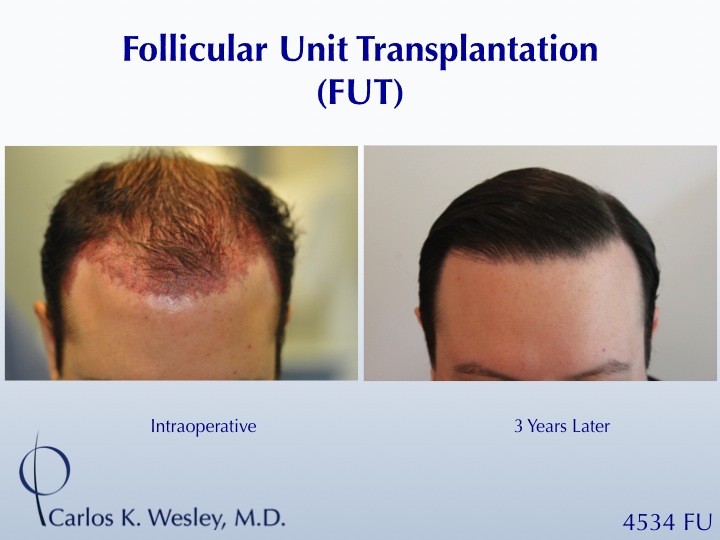
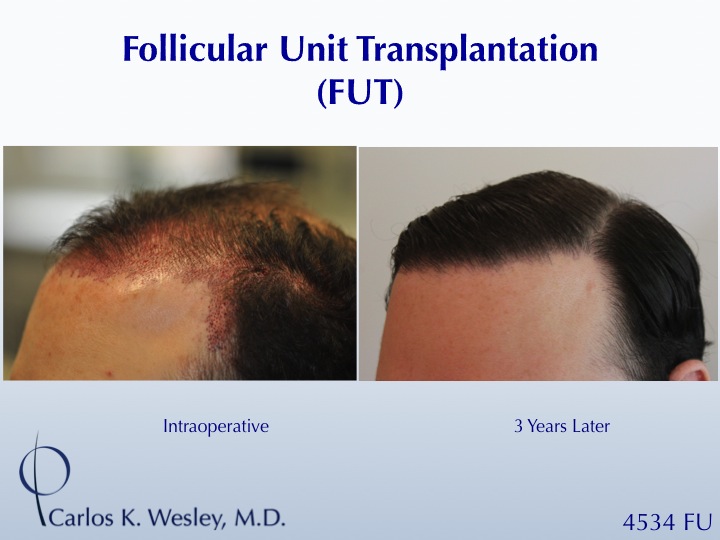


Carlos K. Wesley, M.D. (NYC) - Young Man's Frontal Fullness (4534 FU)
in Results Posted by Leading Hair Restoration Clinics
Posted
Agreed, Bill. We will certainly take and present more overhead images if and when this patient comes back to address his thinning crown.
In general, patients who have ample coverage of the frontal portion of their scalp all the way posteriorly (backwards) to the "vertex transition point" they are left with a natural appearance that looks full from both the front and the side. The vertex transition point is the region towards the back of the head where the scalp begins to slope downwards. Coverage back to this point with a feathered, concave arc of a border allows the transplanted pattern to match the border of any naturally-occuring thinning in the crown. That way, patients are never obligated to return for another transplant simply to make it look natural. Instead, they have the choice of filling in the crown or leaving it thin with a natural-appearing border.