

Dr. Raymond Konior
 Elite Coalition Physician
Elite Coalition Physician
-
Posts
228 -
Joined
-
Last visited
-
Days Won
4
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by Dr. Raymond Konior
-
-
Why are you asking another patient about instructions when you should be contacting me or my office? That is the most direct route to an accurate response since we will providing your care, not the poster on this forum.
-
 5
5
-
-
On 12/5/2020 at 9:00 PM, stephcurry30 said:
Terrific result. Will the patient be coming in for a follow up to fix his crown??
His goals were primarily devoted to hairline restoration. As of his last follow-up he was happy with his hairline and the appearance of a thinning crown. Should he opt for a second session later in life, an FUE harvest would be recommended because of limited elasticity following the strip harvest.
5 hours ago, giegnosiganoe said:@follically challenged I think what he means is that they placed thicker density in the hairline compared to further back (pretty obvious why one would do that). But also placed thicker density on the left side compared to the right (you can clearly see this in the immediate post-op pics) - this is because the patient would be parting his hair from the left side and so would need stronger density to not show as much skin, whereas the right side can benefit from the combover effect. Very judicious usage of grafts.
You are spot on correct with your assessment. A homogeneous graft distribution with his fine hair would have be certain to leave a less-than-ideal result with a weaker part and hairline. Prioritization of those two areas was deemed high for this man.
2 hours ago, follically challenged said:Interesting. I would have thought this may look strange but it seems to have worked.
Does Konior have a YT channel? Seems good work but cant find much recent stuff about his work...only videos from 8 years ago...Gradient grafting is quite routine for the vast majority of men where achievable densities are anything less than dense-pack. Understand that we almost always graft with an end result that leaves a density deficiency, i.e. we do not restore full density with single-session hair restoration. Strategic graft distribution aims to make a "little" look like a "lot".
-
2
-
-
On 11/5/2020 at 12:18 PM, follically challenged said:
Excellent result. Any results of fine blonde / mousey brown hair that you could perhaps share...? Thanks
Just posted is a fine hair case which contrasts the difference in achievable density between fine and high-caliber hair.
-
This 50 year old male requested hairline restoration along with some conservative coverage in the crown. His exam revealed an advanced pattern of loss and very fine hair throughout the donor area. The limitations of coverage associated with fine hair and an advanced pattern were discussed in detail and a plan was devised to best suit his goals. A 3160 graft restoration was performed with density gradients designed to bias graft distribution in the hairline and left-part. In light of his very fine hair, the strategy of using a thick-to-thin transition along front-to-back and left-to-right vectors was deemed best for his overall needs. Immediate graft placement views demonstrate the density gradient plan that was implemented.

preop front

preop top view

preop back view

planned graft zones front view

planned graft zones left-side view

postop front view 1

postop front view 2

postop front view 3

postop comb-back view front

postop top view

postop back view

postop left-side view 1

postop left-side view 2

postop comb-back view left-side

immediate graft placement front

immediate graft placement crown
-
1
-
-
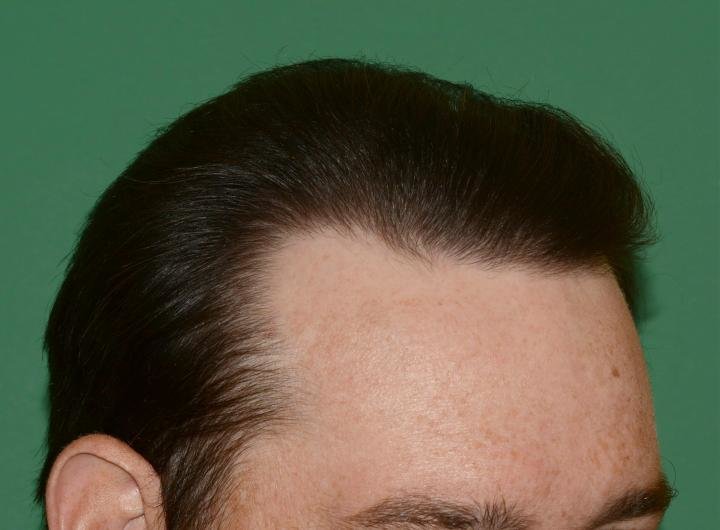
This 37 year old patient presented with a request for frontal hairline restoration. He requested an FUE harvest in order to maintain the ability to wear short hairstyles in the future. A 2092 graft frontal hairline restoration was performed using an FUE harvest. Presented is his seventeen month postop result. Perioperative graft placement photos, along with preop and seventeen month donor site photos are presented. Density inspection photos show the coverage that was obtained in the graft zone.

preop front view

preop top view

preop planned graft zone

postop front view 1

postop front view 2

postop front view 3

postop front comb-back view

postop top view

postop left view 1

postop left view 2

postop left comb-back view

postop right view 1

postop right view 2

postop right comb-back view

density inspection right

density inspection center

density inspection left

day of surgery graft zone

two day postop graft zone

one week postop graft zone

preop donor site

one week postop donor site

seventeen month postop donor site view 1

seventeen month postop donor site view 2

seventeen month postop donor site view 3
-
3
-
-
This 27 year old female patient presented with a request to lower her hairline. She previously underwent a 500 graft FUE procedure, but that procedure was described as a failure in achieving her stated goal. A strip harvest was recommended because of the large graft number needed for her restoration and because she had no intention of shaving her head in the future. She underwent a 3024 graft hairline lowering procedure. Presented here is her eighteen month postop result. Included are immediate postop graft placement photos.

Preop Front

Preop Front Tipped View

Preop Left

Preop Right

Postop Front

Postop Left View 1

Postop Left View 2

Postop Right

Postop Right Comb-back View

Postop Density Inspection

Immediate Graft Placement Front

Immediate Graft Placement Right

Immediate Graft Placement Left
-
This 46 year old man presented with a history of having undergone a 1500 graft FUE hairline restoration. His previous surgeon promised a “no-shave” restoration so as to comply with his desire to maintain an inconspicuous appearance postoperatively. The patient complained that there was little if any density gain from his first attempted restoration. His request upon presentation was to restore frontal coverage and a reasonably defined hairline.
His examination revealed scant frontal coverage with no semblance of a frontal hairline. His donor area revealed two distinct “strips” where FUE harvesting had been performed. Presumably, long hair had been maintained above and below each linear harvest zone for the intended goal of “hiding” his procedure. The grossly unnatural appearance of the donor area surprised and disappointed the patient.
A secondary repair procedure was recommended, once again using FUE harvesting, but designing the harvest to blend the harsh appearance of the donor site scar pattern. A conservative session of 1500 grafts was recommended in an attempt to remain cautious because the etiology of the first session’s low yield was not fully apparent. Of note is that the patient was reluctant to use a shaved approach for the donor harvest, which prompted my comment, “You did that once before and look how it turned out”. Harvesting was confined to areas above and below each prominent FUE-strip-pattern scar. Graft placement was performed using a no-shave, stick-and-place technique. The restoration focused on hairline definition and generalized frontal density enhancement.
Presented here are two-year postop results.

Preop Front

Preop Left

Preop Right

Preop Hairline Plan

Postop Front 1

Postop Front 2

Postop Top 1

Postop Top 2

Postop Top Part View

Postop Left 1

Postop Left 2

Postop Left 3

Postop Left Comb-back View

Postop Right

Postop Right Comb-back View

Preop Donor View

Immediate Postop Donor View

Immediate Graft Placement View
-
On 6/5/2020 at 4:50 PM, HTHope said:
Dr. Konior
what are examples of intrinsic healing predispositions that compromise graft survival ?
One would first have to consider the possibility of compromised graft growth arising from an intrinsic scalp scarring disorder such as lichen planopilaris where the skin essentially attacks the follicles with an end-result of low yield. Also, his history of multiple procedures most definitely had to be taken into consideration in that the many scars resulting from plugs, FUE grafting and the scalp reduction would have compromised his baseline scalp circulation. An aggressive graft plan could have been associated with a higher risk for low yield in the face of diminished baseline scalp circulation. The risks associated with a fast-track approach are unacceptable, especially when graft supply was considered tenuous at best, when a more deliberate and strategic approach would in theory increase the odds of a high graft yield, maximized coverage based on desired hairstyle, and a non-depleted donor area.
-
3
-
 2
2
-
-
On 5/29/2020 at 8:29 AM, experion said:
Very nice results...any benefit of splitting over two and half years instead of 3-4 days continuously?
This restoration was performed over one and a half years, not two and a half years. There was a one year interval after its completion which is when the final photos were obtained for presentation here. There is no reason any ethical surgeon would force a fast-track restoration. First, the patient had been operated on by several physicians with nothing positive to show in terms of graft survival. An experienced surgeon would first question whether the patient had some intrinsic healing predisposition that compromised graft survival. Committing to a one-shot restoration would have proved disastrous should his limited supply have been fully depleted with a resultant low yield as had been experience in his prior procedures. Second, he had a highly compromised donor site with extensive scarring and lower quality residual follicular-units. Attempting the one-shot approach would have risked an over-harvest of the scalp’s donor area with the potential for unacceptable visual thinning and detectable scars. Finally, a staged approach allows the surgeon to strategically build zones of coverage and density gradients based on the perspective of seeing what a prior procedure was able to accomplish. Understand that we are using a relatively small number of hairs to hide a vast expanse of scalp. It is the strategic integration of hair using density gradients, graft insertion angles and prioritization of placement zones that makes a little look like a lot.
Thanks for all comments.
-
10
-
1
-
-
This 50 year old man presented with a history of multiple failed hair restoration procedures. At a young age he underwent several large-graft plug sessions and a midline scalp reduction. He reported that the majority of the plugs failed to grow and what did grow left him with unnatural patches of pluggy hair. The scalp reduction resulted in an exposed midline crown scar. More recently he gained knowledge about the use of FUE and underwent a large session hoping to enhance his appearance. Unfortunately, the FUE restoration proved to be a failure with no apparent graft survival. Sadly, his scarred and unnatural looking scalp had committed him to a life of wearing a hat or hair piece at all times.
His examination revealed a small zone of plug hair in the right and left frontal hairline. The bald frontal scalp showed evidence of many “empty” or nearly-hairless plugs, as well as a large number of small, hairless scars, these a result of the failed FUE procedure. A midline scalp reduction scar was obvious. The donor area was heavily compromised with extensive scarring demonstrated by multiple four-millimeter circular scars from the past plug harvesting and multiple one-millimeter circular scars from the more recent FUE harvest. Although his donor elasticity was judged adequate for strip harvesting, the classic central donor harvest zone demonstrated moderate to extensive circular scarring, as well as poor quality residual follicular-units, these a result of collateral damage from past plug harvesting and his most recent attempt at an FUE harvest. Fortunately, he revealed good quality hair in the chest and beard regions.
Recommendation for repair was made which proposed use a multi-stage, prioritization plan to restore hair with the frontal region having the highest priority and prioritization decreasing in a front-to-back fashion moving toward the crown. The plan proposed an initial salvage strip harvest in the lax but scarred central donor area, followed by FUE using selective harvesting from scalp areas continuing to have accessible follicular units and supplemental body harvesting from the chest and beard areas.
Presented here is a chronological review of his initial four-stage repair.
Session One - August 2017: 2700 Grafts (2400 Strip / 300 Chest FUE) – Front and Midscalp Placement
Session Two – January 2018: 1550 Grafts (700 Chest FUE / 850 Scalp Temple Region FUE) – Crown Placement
Session Three – July 2018: 1160 Grafts (1160 Scalp FUE) – Front and Midscalp Placement
Session Four – February 2019: 1300 Grafts (900 Scalp Nape Region FUE / 400 Chest FUE) – Temple Points, Left Part and Crown Placement
Postop Final Pics – One year from the final session; two and one-half years from the first session.
Comment:
Grafts harvested from the scalp were deemed lower quality because of the extensive prior harvests causing residual scarring in the central donor region and collateral damage to the remaining follicular-unit donor population. Chest hairs, although considered excellent with respect to texture and color, were predominantly low-caliber, single-hair units. Despite these quality issues, the patient was able to achieve adequate density and coverage such that he now lives a comfortable life without any need for a hair piece or hat. Future restorations using additional chest hair and beard hair are in the making.


Preop Top View

Preop Back View

Preop Left

Preop Right

Hairline Plan

Graft Zone Plan

Day of Surgery Graft Placement

Two-Week Postop


Five-Month Postop Front

Five-Month Postop Top

Session-Two Graft Zone

Session-Two Graft Placement

Session-Two Body Donor


Preop Session-Three Front

Preop Session-Three Left

Preop Session-Three Back

Preop Session-Three Top

Session-Three Graft Placement


Preop Session-Four Front

Preop Session-Four Tipped View

Preop Session-Four Top View

Preop Session-Four Part View

Session-Four Graft Plan View 1

Session-Four Graft Plan View 2

Session-Four Part Graft Placement

Session-Four Temple Point Graft Placement

Session-Four Crown Graft Placement


Final Result Front View 1

Final Result Front View 2

Final Result Left View 1

Final Result Left View 2

Final Result Left View 3

Final Result Left View 4

Final Result Left View 5

Final Result Left View 6

Final Result Right View

Final Result Top View

Final Result Back View
-
3
-
-
This 50 year old patient requested hair restoration. A total of 4114 grafts were performed over two sessions using FUE harvesting. First session grafting concentrated on the hairline and temple points. Second session grafting focused on transitioning frontal reinforcement into the midscalp and crown. Presented are one year postop pics along with immediate postop views of the graft placement.

Preop Front

Preop Left

Preop Right

Preop Crown

Planned Frontal Graft Zone

Postop Front

Postop Front Comb-back View

Postop Left

Postop Left Comb-back View 1

Postop Left Comb-back View 2

Postop Right

Postop Right Comb-back View

Postop Donor Area

Postop Top View 1

Postop Top View 2

Postop Top View 3

Postop Top View 4

Postop Density Inspection Right

Postop Density Inspection Right-Center

Postop Density Inspection Left-Center

Postop Density Inspection Left

Session 1 Graft Placement Top View

Session 1 Graft Placement Left

Session 1 Graft Placement Right
-
This is a 34-year old patient with a history of undergoing a frontal hairline flap using tissue expansion of the left donor region. He presented to my office with complaints of an abrupt hairline, a frontal hairline scar, an unsightly left-side donor scar, and thinning in the midscalp and crown regions. His primary goals were: 1) create a more natural hairline; 2) camouflage scars along the hairline and in the donor area; and 3) enhance hair density in the midscalp and crown.
His physical examination revealed:
1. An overly-thick frontal hairline flap with backward-oriented hair.
2. A disfiguring, hypopigmented scar that traversed the entire length of the hairline.
3. A prominent 1 cm scar in the left and back donor areas that traversed the path of the previously transposed hairline flap.
4. Significant density reduction in the temple region surrounding the transposition point of the flap.
5. Advanced miniaturization in the midscalp and crown.
6. A clinically apparent scar along the back edge of the flap.
7. Disproportionate thinning in the lower left crown which had resulted from this edge being displaced downward during closure of the flap’s donor defect.
Surgical Plan: The entire left donor area and left occipital region were eliminated from consideration for donor harvesting because of severely limited elasticity and density reduction that resulted from removal of the flap and because of the preexisting wide scar. In anticipation of a large graft requirement to accomplish the many goals at hand, a multi-stage approach was developed that would begin with strip harvesting and later convert to future FUE harvesting once the donor region elasticity threshold had been fully utilized to preclude any additional strip harvesting. The right temple and occipital donor regions demonstrated sufficient density and elasticity to allow strip harvesting for the initial stages of this restoration.
Result: Presented here is the result of two graft sessions that were staged seven months apart and utilized a total of 3,685 grafts procured via strip harvesting. Session 1 consisted of 2292 grafts, distributed into the frontal hairline scar region, the occipital scar, and the midscalp region. Session 2 consisted of 1393 grafts that were distributed into the crown, a gap located between the right end of the flap and the adjacent temporal hair, the right hairline scar, and a thinning left-side donor area surrounding the flap’s transposition point. Postoperative photos demonstrate results nine-months following the second session. Additional density gains are expected.

Preop - Front

Preop - Left

Preop - Right

Preop - Top

Preop - Back View

Planned Graft Zone - Front

Planned Graft Zone - Midscalp

Planned Graft Zone Session 2 - Crown

Postop - View 1

Postop - View 2

Postop - View 3

Postop - View 4

Postop - View 5

Postop - View 6

Postop - View 7

Postop - Top View

Postop - Back View 1

Postop - Back View 2

Flap Donor Scar - Anterior

Flap Donor Scar Graft Placement - Anterior

Flap Donor Scar Result - Anterior

Flap Donor Scar - Posterior

Flap Donor Scar Graft Placement - Posterior

Flap Donor Scar Result - Posterior

Graft Placement - Front Hairline

Graft Placement - Crown
-
1
-
-
On 1/1/2020 at 12:55 AM, yesplease said:
Very impressive.
What is the patient’s age? Is he on medical therapy?
The patient was 45 years of age at the time of surgery and originally presented to my office with a history of using finasteride and minoxidil.
-
This 45-year old patient presented to our office requesting enhancement of his frontal hairline. He underwent a 3100 graft frontal hairline and temple point restoration using strip harvesting. Presented are his 22 month postoperative pictures. Immediate postop views demonstrate his graft placement.

Preop Front

Preop Right

Preop Left

Planned Hairline Front

Planned Hairline Right

Planned Hairline Left

Postop Front View 1

Postop Front View 2

Postop Front View 3

Postop Front View 4

Hairline Comb-back Front

Hairline Comb-back Right

Hairline Comb-back Left

Hairline and Temple Point Inspection View

Recipient Site Density Inspection View 1

Recipient Site Density Inspection View 2

Donor Site Scar

Intraop Graft Placement Center

Intraop Graft Placement Right

Intraop Graft Placement Left
-
14 hours ago, stephcurry30 said:
Dr. Konior,
I was researching about HT to the donor strip scar and in certain cases, the grafts placed in the scar don't grow sometimes.
Which cases is this research referring to?
It is also possible for grafts not to grow in the healthiest of scalps, but this is most often a result of poor technique. A poorly harvested or poorly placed graft will be at risk for low survival regardless of where it is placed. My experience shows that donor scars can be successfully grafted as long at healthy grafts are carefully placed in a strategic fashion. If you have any concern about graft growth, it may be wise to consider a small test session to evaluate your growth rate. A test session guarantees that you will not waste donor supply should you have a predisposition to poor growth.
-
This 50 year old patient requested frontal hairline restoration. He underwent a 2200 graft session using FUE harvesting in accordance with his request to have the option of wearing very short hair styles. Presented here are 18 month postop pics along with immediate postop views of the graft placement and two-week postop views (provided by the patient).

Preop Front

Hairline Plan Front View

Hairline Plan Tipped View

Hairline Plan Left

Hairline Plan Right

Postop Front View 1

Postop Front View 2

Postop Top View 1

Postop Top View 2

Postop Front Comb-back View

Postop Left

Postop Left Comb-back View

Postop Right

Postop Right Comb-back View

Immediate Graft Placement Top View

Immediate Graft Placement Right View

Immediate Graft Placement Left View

Two-week Postop Front View

Two-week Postop Right View
-
1
-
-
On 5/31/2019 at 6:25 PM, paddyirishman said:
Why did the patient not op for total FUE?
.........Paddy.....
Point 1: The primary advantage of using FUE over strip for a graft harvest is to allow a patient the option of wearing a very short hairstyle. This patient presented with two prior strip scars, one of which was exceptionally wide. His preexisting donor scars will always prevent him the option of wearing a very short hairstyle, thereby eliminating the decision to utilize FUE as the primary harvest method for his restoration.
Point 2: A secondary reason one would choose FUE over strip for the graft harvest is relative donor site tightness, i.e. a very tight scalp will not allow for strip harvesting. This patient demonstrated sufficient looseness in an ideal location of the higher quality donor area, thereby making strip harvesting a viable option.
Point 3: Planning a procedure has to take into consideration both long term and short term needs. This patient has an advanced pattern with a disproportionate imbalance between his limited donor supply and the high number graft needs of his large bald zone. A key issue here is what harvest strategy would allow this man the opportunity of yielding the largest number of grafts over his lifetime. An aggressive FUE harvest that would have yielded the same number of grafts as this combo approach could have resulted in a “one-and-done” session as the diffuse density reduction associated with FUE-only harvesting may actually have worsened his ability to camouflage the preexisting donor scars. Also, using an FUE-only approach would have forced the harvest into more unfavorable zones at risk for future thinning.
Using a strip harvest for the primary harvest modality in this combo approach has not resulted in any new hair style requirements as the final scar heal from the session presented here was very good, i.e. his current hair style requirement is still based on the prior procedure scar issue. Additionally, the strip harvest concentrated graft isolation from the highest density and best quality central core of the donor area.
In summary, the combo approach maximized a single-day harvest in terms of graft number yielded and overall graft quality, and it has allowed for another future session by preserving residual follicular-unit distribution in the donor area. A future session, however, may very well require an FUE-only approach if the limits of his donor area elasticity have been reached.
-
3
-
-
This 39 year old patient presented with a history of two prior unsuccessful hair transplants in which a total of 3086 grafts had been placed in an attempt to restore his frontal male pattern baldness. He expressed concern that the procedures failed to produce any substantial regrowth or density gain. He was also bothered by a very wide scar that resulted from his second strip harvest procedure.
The prior transplant zones demonstrated quite low density in consideration of the prior 3086 grafts that had been performed. His donor area revealed a very wide scar extending from the occipital region to the right temple donor region. Overall his donor area was deemed compromised because of the past harvests and the resulting wide scar. The surgical plan devised included another strip harvest in the remaining higher density, core donor region, and a secondary FUE harvest for recruiting grafts from the nape region. This combination approach was used to maximize the graft harvest while minimizing further cosmetic handicap in the donor region. The strip harvest yielded 2829 grafts and the FUE harvest yielded 541 grafts, resulting in a total of 3370 grafts for the restoration. Strip grafts were primarily distributed in the frontal and midscalp regions, while the finer nape hairs were used to create a transitional thinning appearance from the midscalp into the crown. Presented here are nine month postoperative results. Also presented are various photos of immediate graft placement and the harvest zone.

Preop Front

Preop Top 1

Preop Top 2

Preop Top 3

Preop Left

Preop Right

Postop Front

Postop Top 1

Postop Top 2

Postop Top 3

Postop Left 1

Postop Left 2

Postop Right

Planned Graft Zones

Immediate Postop Strip Graft Placement View 1

Immediate Postop Strip Graft Placement View 2

Immediate Postop FUE Graft Placement

Immediate Postop Combo Graft Placement

Immediate Postop FUE Donor Site Appearance

FUE Donor Site 24 Hours After Surgery
-
On 5/10/2019 at 3:33 AM, Dhyan said:
Dr k. What are the best grafts to conceal SCAR, scalp or beard ?
There is no single best source for all patients. Hair color and texture matches are important, and it is not uncommon for these characteristics to vary between the donor and recipient sites. Beard hair is a good option when the scalp shows signs of donor depletion and the physical characteristics of the two zones are relatively favorable. Hair for hair, beard is a good camouflage agent because of its high caliber. Each patient needs to be evaluated on an individual basis to determine what is best for him or her.
-
1
-
-
This 36 your old patient requested density enhancement in his centralized frontal and midscalp thinning zones. A total of 1918 grafts were used to boost density in his priority zones. Presented are sixteen month postop photos.

Preop Front

Preop Right

Preop Left

Preop Top

Postop Front

Postop Top

Postop Right

Postop Right Tilt View

Postop Right Comb-back View

Postop Left

Postop Left Tilt View

Postop Left Comb-back View

Density Inspection Right-of-Center

Density Inspection Center

Density Inspection Left-of-Center

Immediate Postop Graft Placement

4-Day Postop Back Donor Area

4-Day Postop Side Donor Area
-
This 38 year old patient requested density enhancement in his thinning frontal and midscalp regions. His exam revealed a diffuse thinning pattern throughout the male pattern zone. The donor area showed low caliber hair and evidence of retrograde alopecia. He underwent a 3088 graft restoration of the frontal and midscalp regions. Presented are fourteen month postop results. These include part views in the graft zones that demonstrate his density enhancement.

Preop Front

Preop Top

Preop Right

Preop Left

Postop Front 1

Postop Front 2

Postop Top

Postop Right 1
Postop Right 2

Postop Right 3

Postop Left 1

Postop Left 2

Density Inspection Center

Density Inspection Front

Density Inspection Right

Density Inspection Left

Postop Donor Area

Immediate Postop Graft Placement
-
Why are you dying the hair? It's going to be clipped with a zero guard. A responsible surgeon will dye it to the extent that extraction quality will be maximized.
-
The patient should not be worrying about dying the hair if the plan is for a buzz-cut FUE harvest. Dying long hair that will be clipped is pointless as the hair will continue to grow after it is dyed. If the procedure is a few days after the dye, all that will be left for the surgeon to see will be a white stubble. Also, even professional dyes have a hard time getting to the base of the hair shaft. The surgical team should dye the white stubble after buzzing and before harvesting. This easily colors the stubble to show hair direction and angle, thereby making extraction as easy as with dark hair. The attached file shows snow-white hair which was dyed immediately prior to the harvest. The hair shafts are quite easy to see.

-
2
-
-
What is my opinion on clinics that utilize technicians for extracting grafts? Hmm…
Answer these three questions:
1) Would you allow a tech to remove a brain aneurysm on your mother?
2) Would you allow a tech to perform coronary artery bypass on your father?
3) Would you allow a tech to remove a testicular cancer on you?
If the answer is “yes” to any of these questions, you should do nicely in a tech-driven hair restoration facility. If, on the other hand, you answered “no” to all questions, then ask yourself why you would allow a technician to perform a surgical procedure on your scalp. Also, if you answered “no” to all questions, and you decide to use a facility that uses technicians for graft extraction – without direct supervision by the operating doctor – ask your doctor why he or she is not performing the procedure, but rather uses the service of a technician to perform what I deem to be a surgical procedure. Questions I would direct to the physician if he or she uses technicians for graft extraction without direct doctor supervision:
1) Do you use a technician because you have poor eyesight?
2) Do you use a technician because you have a tremor?
3) Do you use a technician because you will be in another room maximizing your profit for the day?
4) Do you use a technician because you don’t believe patient care and supervision is important?
5) Do you use a technician because you are lazy and prefer to surf the web or check your stock portfolio?
6) Do you use a technician because you lack surgical skills and believe the technician is capable of delivering a better quality graft than you would be capable of delivering?
7) Do you believe harvesting grafts is a “simple” component of the surgical procedure or that harvesting grafts is “no big deal” such that it can readily be delegated to a technician?
The bottom line is that I believe hair restoration is a surgical procedure that should be performed by a doctor. It is not a mundane and simplistic task that is capable of being delegated to the technician level. Face it, most technicians have little to no formal education, i.e. they receive “on the job” training. Who is training them and who is supervising them? We in this practice respect the doctor-patient relationship and feel that the patient is entitled to the doctor’s presence in the operating room from beginning to end.
-
6
-







































































































































































































































































2173 grafts Dr Konior
in Hair Transplant Reviews
Posted
The question relates to an inquiry regarding postop instructions, which forum members do not have access to. Written postop instructions are unique to an individual practice and are precise in nature. Patients are advised to follow instructions provided by their surgeons to assure the best result possible.