

Dr. David Josephitis
-
Posts
66 -
Joined
-
Last visited
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by Dr. David Josephitis
-
-
Things have settled back down for us at the office, so I thought I would recap a bit about the 2015 Chicago ISHRS Conference as it is now a few weeks ago already. As you all have most likely heard, the conference was very well attended and had many new and interesting talks for the beginner and advanced hair surgeon alike. A major topic of the meeting had to do with the risks and benefits of doing FUE vs. FUT (aka strip, FUSS). It appeared to us that FUT may not be dead yet, and that there is a place for FUT just as there is for FUE. Dr. Ron Shapiro and I had been working on a study with the risks and benefits of FUE in mind, and I was honored to be able to present it at the conference in the opening session. The title of the talk was: A side-by- side study of 20 consecutive FUE patients comparing the use of a 0.9mm sharp vs. dull punch. I wanted to give the community a summary of our most interesting findings. The complete study will hopefully be published in an upcoming issue of the FORUM journal for hair transplant physicians.
Introduction:
It is challenging to study graft survival and the overall growth of transplants. There have been studies done for FUT which have shown very high survival rates. The survival rates of FUE, on the other hand, have not been studied as well. And comparing the two has also been a challenge. We know that years ago the results of FUE were not as good as they are today. We also know with modern FUE techniques and the increased experience of physicians today that the results are much better. Many practitioners today actually tout that the results are just as good as those of FUT. We thought a good place to start looking was at FUE punch types. There has been much controversy over the type of punch over the years. There are manual, motorized, and robotic FUE. There are different techniques and types of equipment within those as well. One thing that all of those types have is that they employ either a sharp or a dull punch (aka blunt).
Study Design:
We used 20 consecutive FUE patients and made 200 attempts with both a 0.9 dull and sharp motorized punch. We tattooed and photographed the area. While most of our results were immediate (we looked at the data), we also wanted to compare how the donor looked after it healed comparing one to the other. For all the patients, we were looking at transection rate, hairs per graft, yield, speed, and scarring. We also recorded various characteristics of patients looking at age, follicle length, hair curl, skin texture, and so on. We wanted to see if one patient fared better with one type of punch over another.
Results:
Transection rate. Transected grafts are those that have one or more hair cut. This cut can be anywhere along the length of the hair. Basically, it is not perfectly intact like a non-transected hair. This was the most surprising of our results. Initially, we had our staff record all of the data (transected hairs, grafts) as they had been doing for us for years. We were quite pleased with our initial results, as we were getting transection rate of less than 5% for the sharp and less than 2% for the dull. Sometimes, we were even getting rates less than 1% for the dull. We were very pleased with ourselves as we were doing what others in the field were doing if not even better at times. We decided to look even closer at those transected grafts. At same time, we had to change the way we documented our grafts. We used a dedicated technician to only record what she saw and to then pass the grafts on to others to be counted and sorted as usual. When we did this our numbers changed dramatically. Our transection rate was around 20% for the sharp and around 6% for the dull. The percentage increased because we were looking at every single hair that was transected. Other physicians with much lower percentages may not be recording these transections in this careful of a manner. It was quite a difference from our original data. Having done FUE with excellent results for many years at Shapiro Medical Group, we had old data from which we could draw. We thought, as with all of hair transplantation, that experience might play a part. We checked our data from almost a year prior with the data from the most recent cases and there was no change. Now, although these percentages look much higher, we are still uncertain how important these transected hairs are. Many physicians believe most of these hairs do grow back.
Speed was an interesting finding for us. We thought the sharp punch would be slightly faster in extraction but it wasn’t as each type was actually the same. For sharp we found an average of 22 minutes (537 grafts/hour) while with the dull we also got 22 minutes (540 grafts/hour) to obtain 200 grafts.
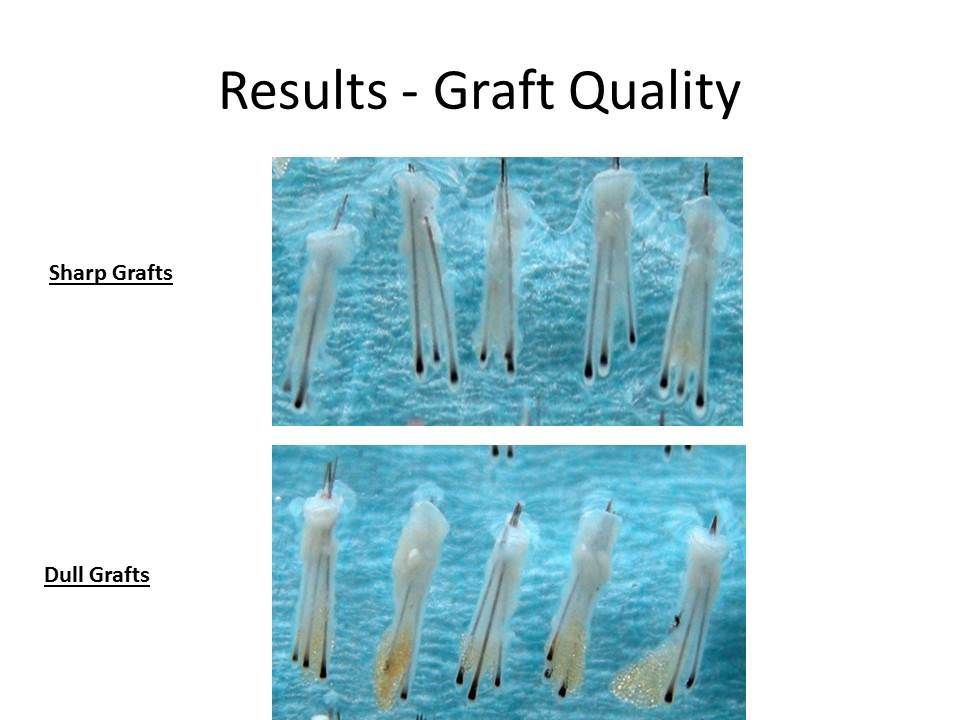
Scarring and Graft quality was looked at as well comparing both types. We tattooed an area so we could accurately find the same spot on the patients’ follow up. In addition to the scarring, we also looked at the general quality differences in the two types of punches. A couple of photos are included below that show how a majority of the dull grafts had more subtle fatty tissue below the bulbs of the grafts. Now, in some of the cases, there was virtually no difference between the two. As a rule though, we found more tissue with the dull punch. Also, below are a couple of photos of a patient with a closely cropped haircut. There is no difference here to be seen with the naked eye. On closer observation though, the dull appears to be spottier than the sharp. Again, for some patients, this magnified view showed no difference. The majority though, showed this slight difference.


Conclusion:
Transection rate appeared to be higher in the sharp punch group compared to the dull. We still are unsure of how important this difference is. Many of the transected grafts may and do grow well in the donor and recipient area. At this time, we are unsure of how many of these grafts grow back. The speed was the same for both groups. Scarring was not very noticeable for both groups, but the sharp group tended to be a little less obvious. This might be because there were more transected grafts in this group.
This study doesn’t immediately change the way we perform FUE at Shapiro Medical Group. We will continue to use the techniques and instruments we feel are most appropriate for each patient. We also use what we know will be in the patient’s best interest giving the optimal results. Some patients will benefit from the use of the dull punch, while with others the sharp punch may give better and more consistent grafts.
This is a thought provoking study which does show differences in different types of instruments. In the future, we hope to use the patient characteristic data that we also recorded to see if one type of patient would benefit from one type over the other. It would be helpful to know this information before we even begin the FUE procedure.
-
Rob,
You may or may not have folliculitis. Folliculitis is an actual inflammation of the hair follicles. It is quite common after surgery to have an area of redness. Most of the time this is just the areas of graft insertion healing. Did you just start to get this redness or has it been going on for some time?
If it is quite new, it could be just that the outside shaft of the hair transplants themselves have just broken off and fallen out. As you may know, this is normal and the root or follicle is still within the skin and is dormant for a time until it starts to grow again in a month or two into a new hair. You may just be having a slight irritation of the skin secondary to the hair breaking off and now the skin in healing over that.
It may benefit to send some photos along to see if you are having distinct areas of inflammation or worse yet ,folliculitis. For both cases, I would recommend washing your hair well every day with shampoo. Make sure you are doing a good job of cleaning the area of grafting. Many patients are too cautious of the grafted area even months after surgery. There is no risk to the grafts a month out.
Also make sure you are keeping the area clean throughout the day by wearing a hat if you are working or playing in a dirty or dusty environment. Finally, try applying antibiotic ointment to the worst offending areas of redness at least once a day for about a week to ten days. This will help to reduce the inflammation. If you are having pain in the area or there is discharge from the grafted area, you should see your physician. They may recommend an oral antibiotic.
In answer to your final question, this should not affect the overall result.
-
Alex85,
From your one week post- op pics, it does not appear that the donor was over harvested. The FUE sites actually look appropriately spaced. Even though there was not a large area of your donor used for the procedure, you had a relatively low number of grafts removed in one session. If you had a greater need for grafting, in my experience, we could have yielded 2500+ grafts over your entire donor area in the span of two days.
I believe the choices you gave of #2 and 3 may be more in line with what is actually occurring. Some people's follicles are more susceptible to shock loss than others. I believe this is what we are seeing. It may take a few months before the donor area returns to normal.
How is the Recipient area in front responding?
Some physicians advocate the use of laser treatment and/ or minoxidil at this time to try to speed up the regrowth of the donor.
-
Hi all,
I thought I'd give a quick update. I'll add a picture taken at 7 mos after my fue surgery with Dr. Josephitis. I haven't experienced as much growth from month 6 to 7th as I did from month 5 to 6th. Is this normal? Should I be expecting more growth or is this the best I can hope for. I'm not knocking the procedure nor am I disappointed in any way. I know it's a tremendous difference from my pre-surgery status. I'm just wondering if I will get more growth in the coming months since I got so much growth in the first 6 months.
I'm glad to see things are looking better for you. The first few months are the most difficult months after surgery, as you can only wait and you don't yet see any of the results. It is perfectly normal to see much more of a change when you did around the 5 to 6 month mark. Even though you don't see much change at this point, it doesn't mean there is no more to come.
For most patients, we tell them that they should not expect complete results of the surgery until 12 months post op. Some patients can even expect additional albeit small changes all the way up to 16 months. Having said that, everyone progresses differently and you most likely will also experience additional change in the future. For you, most of the hairs have likely emerged from the scalp. Some of them are still short while others are already long enough to be cut during your normal hair cuts. All the hairs over time tend to get slightly thicker as they grow longer. All these things help to contribute to the overall result.
I guess that was the long answer. The short one is that yes, you should experience some more density over the next few months.
-
Mythroment43,
I appears that you have two issues at this point. First of all, you have hair loss, possibly from thyroid disease which appears to be continuing despite treatment. Secondly, you are concerned with the possibility of shock loss after FUT.
The first issue of your underlying hair loss may not be as simple as you think. If you have not had your hair loss evaluated by a dermatologist specializing in hair or by a hair transplant surgeon, I would recommend doing so. You might actually have other causes for your hair loss. While thyroid disease is a valid concern, your physician may also want to look at your diet, recent weight loss, history of pregnancy, family history of female pattern hair loss, just to name a few. Also, depending on how long you have been on thyroid therapy, you may not yet have benefited from treatment.
The second issue of shock loss has been covered a number of times here, but still for you as all women especially, it is a concern. It can and does happen. For some women it may only be very subtle and for others a great amount of native surrounding hair may shed the first few months after surgery. For the most part, this hair does return over time. Now, some of the fine miniaturized (thinning) hair that sheds may not come back. This is hair that would have fallen out sooner or later anyway. You current history of active hair loss may or not affect how you do with shock loss. Again, derm or a hair transplant doc can help access with a good history and physical exam.
-
starr,
Beard hair can be an excellent source of "filler" hair once you have exhausted all of your available donor hair. Gillenator is correct that you will never want to use it in a highly visible area such as the hairline. Beard hair is still very unpredictable in its yield and in its overall "value" in the final result. In my personal experience, I have found some patients to have had as low as 50% yield with the use of beard hair and as high as possibly 80% in others. Also, some people have very fine beard hair while others have very coarse hair. Even further still, most beard hair grafts contain only single hairs. Some men I have seen have a higher percentage of 2 - haired grafts. You can imagine that more 2 haired grafts might give better coverage than single haired grafts.
I agree, that FUT right now is your best bet to obtain a large number of grafts for your next procedure. You will have to be evaluated by a surgeon for your candidacy for beard transplant. How good of a candidate will depend on the above items I discussed. If you are able to use beard and you do get a good yield, the total number of grafts available range anywhere from 400 - 1000+. You can only get those totals with multiple sessions.
That was the long answer. The short answer is that you should have your beard evaluated by a doc before you make any decisions.
-
Transhair,
FUE would definitely be a valid option for you. With that type of procedure though, you would have to be willing to shave your hair very short and contend with seeing the FUT scar while your hair grows back. Some offices are now offering No Shave FUE, but this usually is a little more costly, more time consuming, and you may not get as many grafts as you might with a full shave.
Having said that, FUT may still be an option for you as well. It would probably be best for a hair transplant surgeon to put their hands on your scalp for an evaluation. Do you recall how many grafts you had the first time around? Also, how many grafts do you anticipate you will need this time?
If FUT is still an option, we like the patient to do scalp stretching exercises prior to the procedure. Believe it or not, these do help somewhat to create more elasticity and enable us to get more hair safely. Also, here at Shapiro Medical, we now use a product called Vitrase for tighter scalps. It is an enzyme that can create more elasticity in the scalp and enable us to safely take out more tissue.
-
mosd,
From the photos you have, it appears that the frontal core area still has good density. If that is true, then I feel you might be able to get away with doing 2000 grafts for your first FUE session. Of course, if you have a little thinning in that core area then you may benefit from more grafts there as well. I am not sure you will want to do much less than this though. You look to have strong coarse hair. You might even benefit from a second FUE procedure a year from now in the same area if you want added density.
The number of grafts needed also depend on the height of the hairline that you want. If you want to be conservative (higher) and keep an natural hairline, then you will use less grafts. I think at your age it is a very good idea to be conservative to use as little of your grafts as you can. Even with the use of preventative meds, you cannot be sure of how much hair loss you will have in the future. It is always a good idea to save donor for later.
-
20 Something,
We don't typically do surgery for young patients like yourself because there have not been enough years for a hair loss pattern to develop. Thankfully though, your case is very unique. It appears that you have very little if any, other hair loss occurring. Male pattern alopecia is still a potential for your future, but at this time it is not obvious. Also, the hair loss that you have is the result of a scar.
I would recommend 1-2 sessions of FUE to the scar area to bridge the gap of your native hair. The reason I recommend FUE is that your future hair loss is still unknown and the surgery required will not have to be very large. (It is tough to see with the pics how many grafts you will need - probably a couple hundred or less) You may do FUT if you desire.
Also, I recommend more than one session, because we would be transplanting into scar tissue and it is sometimes unpredictable. Depending on how the grafts take, we may have to space the grafts out slightly the first session. It may take more than one session to create a density that you are happy with.
-
FUE2014,
Even after 2 weeks, the grafts are "anchored" into the scalp very well. The hairs will typically shed over the course of the first couple of months. The follicle or "root" is still firmly planted and will resume growing over the course of the next 12 months. At Shapiro Medical we typically tell our patients that they can care for their hair in a normal fashion. This means that they can get a hair cut or use clippers on their head without affecting the future growth of the grafts.
Now the scalp where the hair was transplanted is still an area where you should be cautious. This is an area of the scalp we tell patients to avoid getting sun-burned. The scalp tends to burn much faster the first few months after surgery. Also ,you will want to avoid any harmful chemicals such as those that are used in hair dyes. These chemical or physical burns could not only affect the superficial skin, but also hinder the growth of the future grafts.
Bumps and cuts to the scalps if severe, may also damage the underlying transplanted grafts. The potential for hair loss here depends greatly on the type and extent of physical injury to the scalp. Normal bumps and hits to the head with routine activity should not damage any of the grafts.
-
newhair7,
Did you recall the sutures being very tender, or did the surgeon state that it was a "tight closure?" As is often the case with a second or third surgery, the closure can be a little tight in various areas of the donor scar. This is normal for FUT. The area you showed in the pictures is a typical area where hair loss like this can result. You were correct in thinking that this is shock loss from the surgery. Very likely, over time, the hair will grow back and you will have a similar scar in that area as you had for your prior two surgeries. Rarely, there can be permanent loss around the suture line. In my experience, there is typically pretty good return of the hairs that were lost. Unfortunately, you will have to wait another few months for these hairs to return.
The use of minoxidil is not a bad idea. I doubt that any of the loss is from that. Typically, you are right that the miniaturized hairs are the ones that can fall out initially with treatment. Still, minoxidil may help to speed up the regrowth of not only the shock loss on the sides, but also the transplanted hairs on top.
The red marks from the sutures should also resolve over time. The sutures along with the closure after multiple surgeries all help to contribute to the loss of hair. They are not solely responsible.
-
Torn,
To shave or not to shave? This is often a topic of debate amongst hair transplant docs. Some groups will never shave patients' heads believing that the inconvenience to the patient is much too great and also not seeing any real benefit in doing so. Others, always shave and won't proceed without. Here at Shapiro Medical Group, I like to think we do a little of both, customizing it for the individual patient.
You are correct in saying that it makes it easier for the physician and the operating staff to work without any hair in the way. Shaving or not really depends on the individual patient and their needs. The easiest way to try to explain this is to give a few examples of how we approach different patients. If there is a patient that has a fair amount of hair on the scalp and is only looking to add density, we may see if it will be easy to work in between the existing hair. If it appears relatively easy, then it makes most sense to keep the patient's hair intact and to work around it. Now, if this same patient wanted to maximize density and we were going to work with a large number of grafts (i.e.> 2500 - 3500 grafts) then we might encourage him to get it shaved. We feel that first of all, we may not be able to maximize the density with the native hair in the way, and also the surgery will also be longer in duration. Out of body time does become an important factor in larger cases. The difference in the number of grafts placed between a shaved and unshaved patient may only be 200 - 500.
Another example is the patient who has only very little hair on the scalp that is really not helping for any cosmetic coverage. This we will typically trim down as well, as it again makes it more challenging to transplant. This fine miniaturized hair can become matted down and sometimes interferes with graft insertion. These patients typically will not mind us shaving as there was not much hair there in the first place.
Finally, another patient desiring max. density with adequate (albeit thin) hair on top may not be able to cut their hair short because of school, work, or social obligations. We do not have to cut the hair. This patient will be made aware though, that we might have to do slightly fewer grafts. The patient will most likely still get excellent coverage and a nice result. The patient has to weigh the pros and cons.
So put it simply, we prefer to shave for those desiring a large session to maximize the density and to decrease the graft out of body time. Having said that, working around hair in most cases is also possible. Each patient is different and we will discuss what works best for him or her.
-
Experience,
Most likely you have had your FUE procedure within the last few weeks. Occasionally after surgery some of the recipient site can become inflamed and if worse still, infected. My initial recommendations for patients with only a few red and tender areas on the scalp would be to make sure you are shampooing the scalp daily and preferably with an antibacterial shampoo. Also, apply topical antibiotic ointment to the worst offending areas at least twice a day for about a week. Avoid picking or scratching the areas.
Still, after having said this, it is best to follow up with your hair transplant surgeon in the office or on the phone to update them on your progress. If necessary, they may also want to put you on some oral antibiotics.
If you take care of this in a timely manner, there should really be no ill effects on the final FUE result.
-
PeterD,
Mike is right that the transplanted hairs do not always match exactly the surrounding native hairs. The color and sometimes the caliber can be slightly different.
For patients who are already starting to lose the color in their hair, sometimes we can avoid certain areas of the donor when transplanting. For patients like yourself that have not yet gone gray, it is really unknown what your the future distribution of hair color will be.
One positive fact that plays a part in all of this is how the hairs are actually transplanted. When they are sorted under the microscope and finally transplanted into the recipient area they are placed in a somewhat random manner. White hair is mixed with the darker colored ones. This should somewhat assure more of a random distribution of white and natural colored hair in the recipient area for the final results.
With large sessions of FUT and FUE this question of placement of white or non white hairs can be an issue. With smaller sessions in someone who is concerned about it, FUE may be a viable choice. By doing a smaller case, we can select out for only the hairs that still have their native color.
In the end though, most people over the years do lose the color of the hair and after a transplant the final distribution may be unknown. Dying the hair may ultimately have to be done for those who have had a transplant who decide that hair, even though it is graying is still better than thinning.
-
themojitoknight,
Patients usually get transplants for one of two reasons. Some have very thin or bald areas and transplant into those areas to replace what they have lost. Others, like yourself have thinning, but may still be able to somewhat conceal that loss with existing hair. The latter will get an HT because they don't want to be completely bald before they do anything about their hair loss. Both types are great candidates for surgery. The only issue with patients like yourself with native hair still in the area that is to be worked on, is that it is indeed more sensitive to "shock - loss." Thankfully men are less sensitive to this phenomenon than women and rarely lose a large amount of hair. This shock loss usually resolves after a few months and grows back with your transplanted hair. Some of the finer hairs that were already on their way out may not return, but in the end, they most likely did not impact the overall density anyway.
The surgeon's technique can play a part in the occurrence or not of shock loss. It may also be helpful to use minoxidil pre and post operatively as well as low level light therapy. Finally, temporary use of a hair system may be the last resort. After all of this, you may still experience it, and it may just be something you have to be prepared for.
Some patients that start minoxidil have shedding of hair. This is typically a good sign and indicates that the med should have a favorable effect on preventing hair loss and possibly thickening some fine hairs. I would recommend trying it again. You really can't tell if a hair med is actually helping unless you use it for more then 9 months. Unfortunately hair grows very slowly. The dry scalp can be helped by using an antidandruff shampoo once or twice a week or by backing off slightly on the minoxidil (once a day instead of twice). I would try the shampoo route first.
Saw palmetto is unregulated and theoretically should have similar side effects as Propecia. If you want a DHT blocker I would recommend seeing an HT doc and getting their advice on its pros and cons.
Shapiro Medical Group FUE study: Comparing 0.9mm sharp vs. dull punch
in Hair Restoration Questions and Answers
Posted
That is interesting that you mentioned the study between FUT and FUE. During that same ISHRS meeting we received a grant to perform that exact study.
Most prior studies comparing FUE and FUT had been done on a small scale. (100 or 200 grafts) It is more difficult to see a difference with a small study like that. Our upcoming study (when we can gather some willing candidates) will be a full scale study (2000 grafts or more) comparing the two techiniques.
Thanks for the input and stay tuned.