
Zup
-
Posts
111 -
Joined
-
Last visited
Content Type
Forums
Profiles
Store
Gallery
Articles
Blogs
Events
Downloads
Posts posted by Zup
-
-
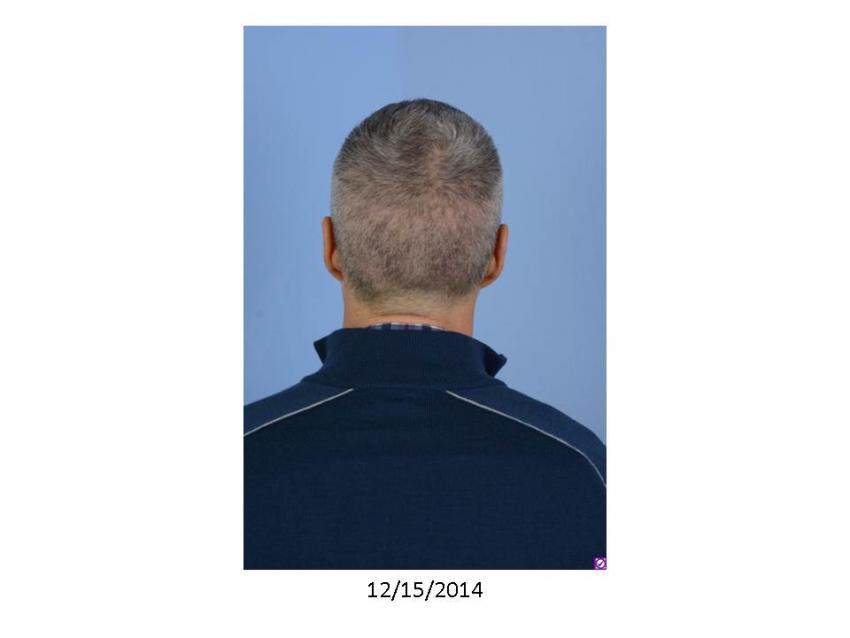
17 days post-op. Hair has grown a bit and not much shedding
Merry Christmas and Happy Holidays to all!!!!





-
Spanker,
I used dermatch for a while, but then a make-up artist from NY, that we worked on, told me about a similar product he used on his clients called Fill-in Powder for Men. The product went on smoother and virtually waterproof, it is a great little product. I never liked the fibers that one shakes on, even though they're more widely used.
I've been on Propecia for 16yrs. first at 35....I am 51 today, minimal side effects possibly a slight film on the libido but nothing else from what I can tell. It is an effective med, in fact I have never seen someone NOT respond to it. One should use it not to grow back hair, but to maintain and thicken miniaturized hairs, especially in the crown. If anything can grow back hair Propecia can, but one should use it more to keep and improve quality of hair, regrowth is bonus.
-
Shampoo
Thanks......but sense it is stated as a question regarding two todays.
If the clinic is going to give it to a patient it is only a benefit I would say. Most clinics would want to do two patients in two days. We are willing to provide two days to take our time. Many cases the second day is back up and we only do a 1/3 or a 1/4 of the work, but it allows us to take our time, not rush and refine on the 2nd day.
Shampoo I appreciate the question?
I can not see a disadvantage to the patient, maybe the clinic.
-
FHT
Thanks for that.....it is actually is a design, because when all my hair was in tacked it was almost straight. And, that's all some seem to want or push for, I always liked a little recession, a bit of a V. It is adds character.
Regards
-
10 days Post-op, at work on Monday...
Most of our patients take off 7-10 days up to two weeks from work. Most of the redness should be gone and nothing should look surgical, having suitable hair style could be a bit longer, 2-4weeks.




-
Hey you guys,
I am in the stay boat now!
4mths is Springtime....that's when you start watching!
Anything before then is coping.....
I tell all patient take your mind off it after surgery and don't even look at it until 4 mths because you are not going to see much of anything.
I know, anytime there is invested interest.....one is going to watch every step.
We are who we are.
Hadenough - Sunnycool.
You contact us anytime with anything.....it is kind of fun, in anticipation!
Happy Holidays, Matt
-
#47......
Thank You......"Young, smart and cool"......I will take that!
I don't mind..........the stealth look!!!!!
Happy Holidays
-
Exactly one week post-op, Friday at work. Happy Holidays!!!!





-
Thanks everyone......
Staggerlee,
I had all three of the doctors' hands on me; I actually scheduled on days Dr. Paul Shapiro does surgery. Dr. Ron freed himself up to be there and our third doctor, Dr. Joe, did the extractions. If I would have only had one of the doctors I feel patients would have asked why I chose him and not the others. Even though I feel I am as picky as any patient I've catered to over the years, I was comfortable with the Shapiro Medical process, in regard to experienced skilled staff, our instrumentation and quality control, that Ron Shapiro has put in place.
Spanker,
Actually, years ago I wanted to do this procedure but Dr. Ron Shapiro and I decided it was best to wait. I had discovered a concealer fill-in powder that gave me everything I was looking for esthetically, was easy to put on and was weatherproof. I was very open and would tell all patients yet most would say, "Why? You have a full head of hair." Well, it was to create the appearance of a full head of hair. At that point I was content and decided to wait until I thinned more and the concealer wasn't working as well.
In my position as an educator, patients are always suspicious and I did not want to do a transplant as a ploy, just to say I had a hair transplant, when 98% of it was my own hair and there were a few follicular units sprinkled amongst it. I wanted to be thin enough to be able to document the level of improvement so patients themselves could see the level of change.
Also, in Minnesota Nov-Dec is really my only window. I am very active Spring through Fall; avid Road Biker and completive Ultimate Frisbee player, in fact this year our team was National Champs and won our 2nd Gold Metal in the last 3yrs.
-
Joe, Thanks for being the first to welcome me. All the very best. Matt
Squatch, It was exactly the comb I was envisioning.....however, they came even a little fancier, where the colors swirled together like a Lava Lamp.
-
My procedure was done last Thurs-Fri, approx. 2150FUs.
I was the guy even in grade school who always had a comb in my pocket making sure my hair was always in place.
I'll be happy to share my story.
Happy Holidays
------------------------------------------------------------------------------------------------------------------------------------
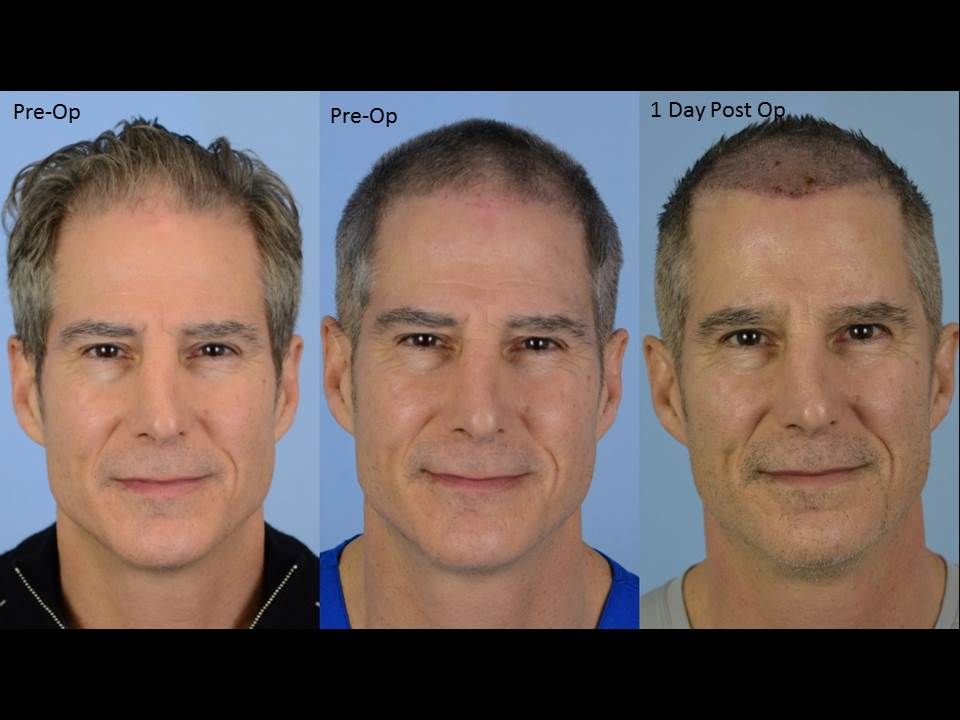
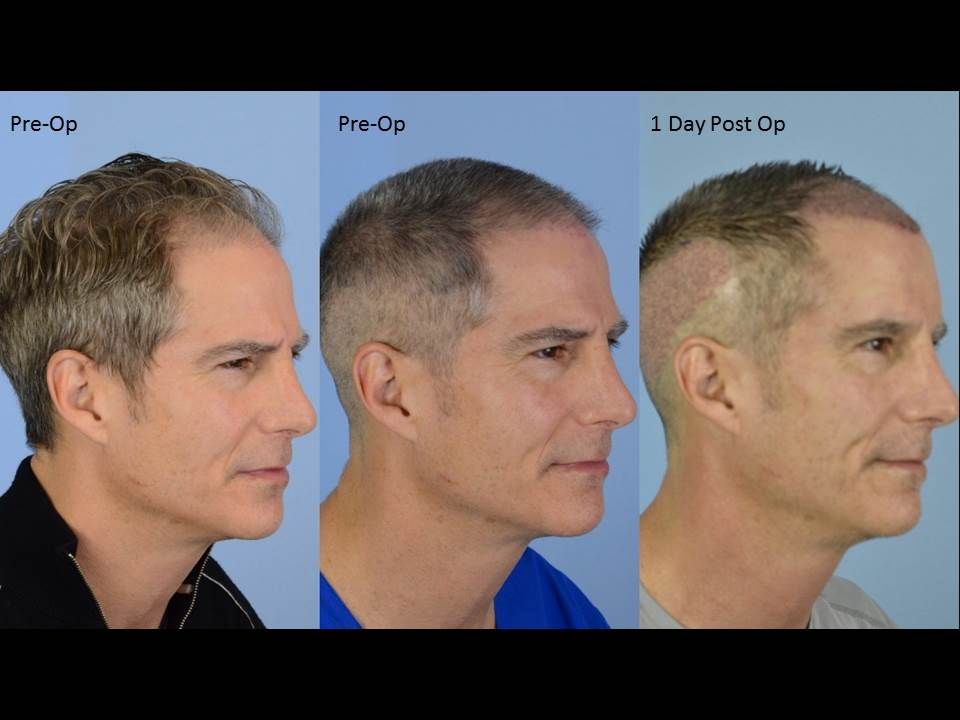
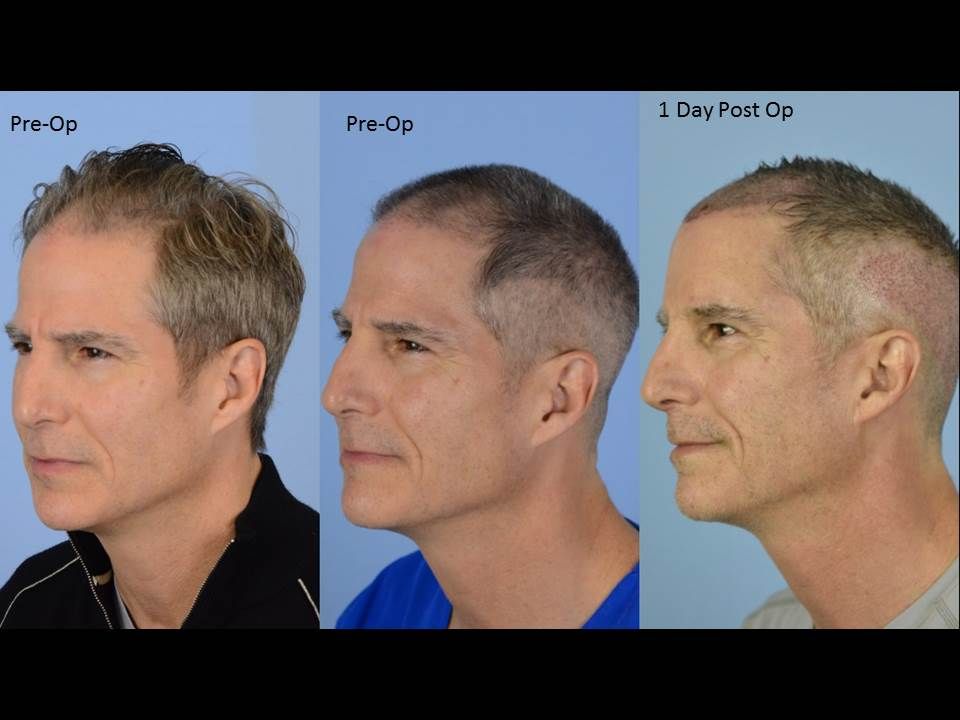
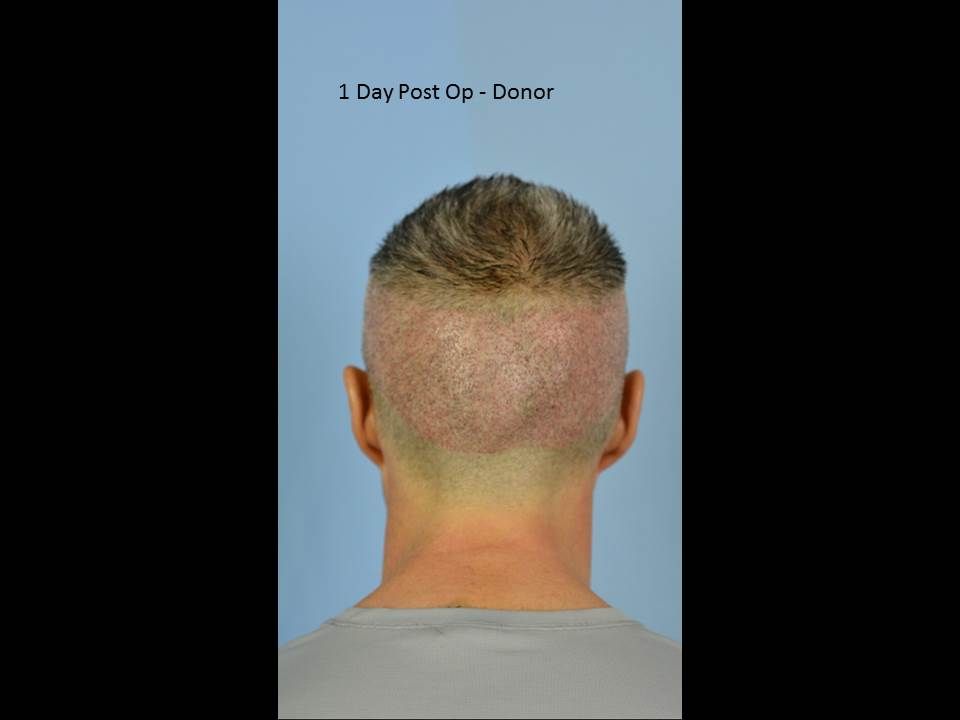
Here are pics put together that show Matt's hair loss before surgery- two sets of pics taken before surgery - one with normal length hair and right after shaving down to get ready for surgery. We kept it a little longer on top, something resembling a military style cut. The third set of pics are 1 day post ops.
Graft/Hair Total & breakdown: 2105gr/4472 hairs
1's - 416
2's - 1078
3's - 544
4's - 67

-
I like it. Nice job. Matt
-
Ash, Yes, that's true......but I said much more.
As well as, I never said the growth appeared fantastic, but uniform, but a little spotty on the hairline and it may fill in yet but if not we'll stand behind it. I also indicated concern, when I said would you like me to set up a phone appointment with Dr. Paul and we should break the next 6 months up into two follow ups not just one, to follow you closely.
We ,however, need to see it through before we act or do anything.
The fact that I believe he may be losing native hair, is his crown is thinner also and no work was done there. Yes, he is on Avodart and that's great, but it still is no guarantee one keep all his hair. The meds works best in the crown and works in the front but not quite a well. Patients can definitely loss hair on meds, it does not mean not to to use them, it buys a patient time. Propecia and Avodart work well, specially initially. I don't believe the meds ultimately stop the problem, like turning off a facet, but more like turning it down and may lose their effectiveness over time.....especially if the hair loss problem is genetically a strong one. It is still away to hedge against progression which is critical when you are dealing with a progressive problem and a limited source. Sometimes the meds just delay things, so rather then losing hair over 5-10 years it 20-30 years. The longer one keeps the native it buys them time for new technology that may work even better.
Ash, will speak with Dr Paul Shapiro tomorrow and we will do everything we can to help and see this through.
-
Hello Mike, You will initially meet with me, Matt Zupan their Patient Educator and assistant. Dr. Ron & Paul are always at the office and are available to come in within the appointment for you to meet and for them to evaluate your condition. You will get various opinions from others, but I really feel both are equally good and consist today. Dr. Paul is great because of Ron, he trained Paul and has set the quality control at our clinic, but Paul is his own man today. I myself have been with Dr. Ron Shapiro, going on 25yrs, ever since he's been doing hair transplants. We all look forward to you visiting our office. All the best...
-
To ones enquiring,
In general, I believe our work at Shapiro Medical is very consistent, with growth on the average of 90-100%, and transection rate manually or with the Artas Robot approx. 3-7%. If transection rates are low and survival is consistently high 90-100%, our FUE should be virtually as good as our FUT, in that the rest of the procedure is the same as FUT. We are a bit more conservative with FUE and we generally don’t do as large of sessions, at this point we would rather add more hair then have issues.
We take the same high level of care in doing FUE as FUT; skilled and caring staff, implementing what we believe is the state of the art equipment and technology, with strong internal quality control. I do not believe anyone is doing anything over us, honestly.
Now, we do not push the numbers, in regard to big FUE sessions that will produce necessary WOW results (big transformation), because of some concerns. The numbers may increase in time, we'll see. I believe our results are of high quality, and usually meet our patients’ goals. Because our sessions are usually between 1500-2500fus, after the work has grown out, patients may feel they may want more. If all a patient ends up needing is a bit more hair, that is not necessarily a bad thing. I understand that patients ideally would like to have their goals met in one session, but goals are subjective and some, because of future progression, may need to accept a result a bit thinner to address other areas adequately down the road. At our clinic I always make sure patients are aware that they may need more work, and this can be the case with either FUE or FUT, but I caution them more with FUE. We try to get our patients where they need to be in density, regardless of the technique, by using no more hair then we have to. This is to ration the donor for the future, and not paint someone into a corner.
I believe the internet has made patients believe that whatever a clinic does (as far as number of grafts) in the first session, it should be the magical number that meets all their goals. That is not the case, as goals are subjective. You could take three individuals that are physically identical, and each may require a different degree of work based on their nature. Like in golf, we don’t think we are going to necessarily sink the ball in the hole 200 meters out, however, we are trying to get it close so that we can hopefully putt it in on the next shot. If it goes in on the first shot it is a bonus. Sometimes, when patients were hoping the results would have been a bit fuller in the first session, they believe something did not grow. This may be the case, but most of the time it is not the case at our group. The patient’s expectations for their preferred density were just higher then what the graft number would achieve, even at 100% survival. It is then also the job of a good clinic to determine, based on multiple factors, if it is safe and appropriate to add more hair based on the degree of future progression anticipated.
Density is really the only matter we ever address at Shapiro Medical, and NOT because of poor growth. It is because unless you can match normal density or exceed it, no patient is ever going to say, “ You gave me TOO much hair.” No clinic has ever heard this from a patient.
We want to meet every patient’s goals regarding high quality and density, but we are also making sure we are saving donor for the future as one progresses.
-
Everything I read seems in line and touches on the principles of coverage and density regarding a type 6 pattern.
As Jotronic mentioned "acceptable" is subjective, ones donor density and characteristics makes a difference, as well and the surface area to the Male Pattern Area.
We have been measuring the MPA (basically the top plane of the head) on our patients for over 12 years. In type 6 patterns the balding is retained to the top plane of the head, vs a type 7 that has left the top plane and receded down on the sides and back, increasing the surface area. We have found the surface area on the average patient is approx 200cm2, and does not vary too much.
Average donor yields approx 4000-8000fus, this is supported by the text books, and many of the long existing clinics experience.
It is actually hard for clinics to know exactly what a patients donor density is, we can usually tell if it is low, if it is not low it is either average or above, and since we don't know for sure we always evaluate what we know the patient has, not what he might have. We do take close up magnified photos and do math to calculate things more accurately, but there are other variables to, so no one real know for sure.
Unless someone clearly has above average density, we are going to base things on moderate, 6000fus.
Now, it is math, average patient who progresses and becomes a type 6, has 6000fus, you distribute 6000fus over 200cm2 that's bald that yield 30FUs/cm2 over the entire pattern. What is 30fus/cm2, depending on one’s hair characteristics; 30FUs/cm2 could be the low end of a fuller appearance. So, that's not bad for someone who would be otherwise totally bald. Now, how most patients would most likely distribute the hair, would be rather then 30fus evenly over the entire head, most would prefer 40fus/cm2 in the front 100cm2 and the crown the back 100cm2, 20fus/cm. 20fus/cm2, is approx a quarter of original density, and may be just enough hair to hide the scalp, when the hair is dry or a coverage that appears as more hair then scalp (but, see scalp), in others cases a film of coverage.
Many men, are not that concerned with the crown, and even the ones that are, they don't have the highest expectations. All they generally need is just enough hair to hide the scalp, anything more doesn't look much different.
Also, concealers as well as SMP, could work as a nice adjunct, and could take a crown where one is seeing as much scalp as hair, to seeing no scalp. If you don't see scalp, things look full.
I hope with the other posts, this helps put a proper perspective on things.
-
FUNNY and THANKS.....
Arrie, Is that YOU, we have not spoke for years!!!!!
Just to let you know, our ULTIMATE "FRISBEE" TEAM won the Gold Medal at NATIONALS this year!
-That's where Zup and my picture came from.....the Ultimate field.
-
I don't know about the "old Dog thing", but I don't always take them....I take a look at them.
When we take photos, which is for the patient's documentation not marketing, they're generally not asking to see it.
When we do take a photo of it, it generally just looks like a part in the hair (which we can provide many examples of), possibly a faint white line in the scalp or some slight disruption in the scalp. If the camera can't detect anything, people may just think the hair is not parted at the scar at all....and are sketical.
When hair is grown out around the scar it is hard to capture....I guess that's the impression most clinics want to convey. I never imply our scars are undectable or invisble. We use a double layer closure usually accompanied by a Tricho closure resulting in a scar that is quite faint. Not allowing one to shave their head, but wear their hair short, usually a 1cm or longer.
If one needs more help, to potentially wear is shorter, one could pursue SMP or FUE into the scar. With both of this rememdies available, few of our patients have requested the need.
Regards,
Thanks, Janna
-
Dr Reed is a very good and very repected doctor in our industry, it would serve you to visit him. Regards, Matt
-
Happen to catch this....so I'll provide a quick response, I am off to my daughters choir concert.
Pupdaddy & Future HT Doctor, are correct.
At SMG we pre- make 85-90% of our recipient sites and then place our FUs into each of these sites, approximately 150-300fus are saved for the end, where Dr Shapiro will make 2-3 passes to tweak and fine tune specific areas (primarily the hairline Zone) with "Stick & Place" (making recipient site, placing the graft one after the other).
Lateral or Sagital sites, are the direction of the incision and, can be used with either Pre-made or "Stick & Place techniques.
Regards,
-
Hey, where did you come from....
Big Attorney Man!!!!!
Nice advice, I thought you may have lost it.....but, you address some strong points.
All the very best....Zup
-
Hey Spanker, good job....things look very nice!!! I can tell a lot at this point and your result will look very refined and natural. I am happy for you, you have been quite concerned and apprehensive in making the right decision. I believe your thorough research and patience paid off. Dr Konior, possess all the necessary ingredients to create the highest quality results. You have also been a great source to many others on HTN, of sound insight, with your many posts. Regards, Matt
-
Davis91, yes this is something we are considering.....we now have meet in person and gathered knowledge from NHI, GLI, and the temporary ink group from Milan. We know this could be a nice adjunct with transplantation for many patients, with the impressions serving to give the appearance of better coverage and density. By doing this in house, we're more in control. Allowing us to plan this out with the patient for the best and safest approach both short and long term; treating and placing each impression as carefully as we do ones limited donor, with the addition of anesthesia. We take time to incorporate new things, so that many of the kinks have been worked out, to minimize added risks to hopeful patients.
Matt
-
Yes, we have been in contact with FTS. We probably would recommend a scar revision, then possibly SMP, but very likely the SMP may not be needed. If one is considering more work in the near future, why do it, other than for a more conservative and temporary fix, in reducing contrast. SMP, without reducing the gap ultimately, in the long run, will not be as helpful, plus when the day comes to do more work the scar is going to reduce the yield.
FTS, as he has indicated had two previous sessions from another clinic, therefore we were dealing with the circumstances of that work. Which was a scar similar to what you are seeing. In many cases we may have been able to yield the grafts needed and reduced the scar. The previous scar was primarily behind his ears and he indicated he did not what to go longer to get the grafts. It was decided to extend it a bit but minimal. The length of the strip is generally not the concern it is the width, that can causes problems.
The scar at this time should not be difficult to improve, possibly to a fine line, which is the case for most of our virgin patients. Industry's standard is 1-3mm. The difference is with a scar revision is, one goes only after the scar tissue, and not for hair also, so the width is less and the tension is less. Nearly a fifth of our work monthly is corrective work, and we restore the great majority of these patients to a very respectable look, but they are not the same as a virgin patient.
Our method of closure is generally a double-layer closure using internal sutures underneath and removable sutures or staple on the outside. This closure maintains the integrity of the scalp above and below and holds the scalp together under more tension. In general this method is capable of producing a finer scar, which should allow most patients to wear their hair quite short, approx. half inch. If there is a desire to try to wear the hair even shorter, FUE into the scar and then possibly SMP could be considered. We have had less than 3% of our FUT patients feel the need to pursue these added measures. With the industry evolving and patients getting pickier and pickier, more may!!!
Regards, Matt















24 yrs in the industry with Shapiro Medical, I just did my 1st H.T with FUE
in Hair Transplant Reviews
Posted
DMS2894
We did approximately 1700fus the 1st day and close to 500fus the 2nd day to blend and fine tune.
These days we are using a motorized drill called Aseptico, which allows us to use either a dull or sharp punch. On me they used a .9 diameter sharp punch. Most of our work is done with .8 and .9 punch size.
Merry Christmas to all